32 year old, caucasian female with extensive bone loss and slight mobility. ASA 2 patient due to smoking 1 pack of cigarettes per day for 9 years. The patient also had a history of a tongue piercing, which could have attributed to the destruction on the lower anterior teeth. After exposing FMS radiographs, I was concerned that scaling teeth #24 and 25 could lead to severe mobility. If this was the case, I would consider leaving some of the calculus deposit acting as a splint until the patient was able to visit a Periodontist. However, after evaluating the clinical attachment and calculus deposit, I was able to go ahead with the dental cleaning. The treatment plan rendered was scaling and root planing, polishing with fine paste and applying NaFl Vanish 5%. I recommended using a microbial rinse for her gingiva, which was red, bulbous, shiny and spongy. In addition, I discussed proper brushing and flossing technique. Flossing was a main concern when dealing with pocket depths. A referral was given for carious lesions on #15-mesial and 31-mesial, as well as periodontal evaluation. I recommended the patient to return in 90 days to examine her progress with home care.
The patient responded in a very positive way. She had not been for a dental checkup for over 10 years. However, through patient education, I was able to convey to her the importance of dental care. She realized that it came to the now or never point for her oral health. She was very motivated to change her oral home care and is planning to implement the tools I introduced to her into practice.

Perio Type III due to extensive bone loss and Grade 3 mobility on #24 and 25.
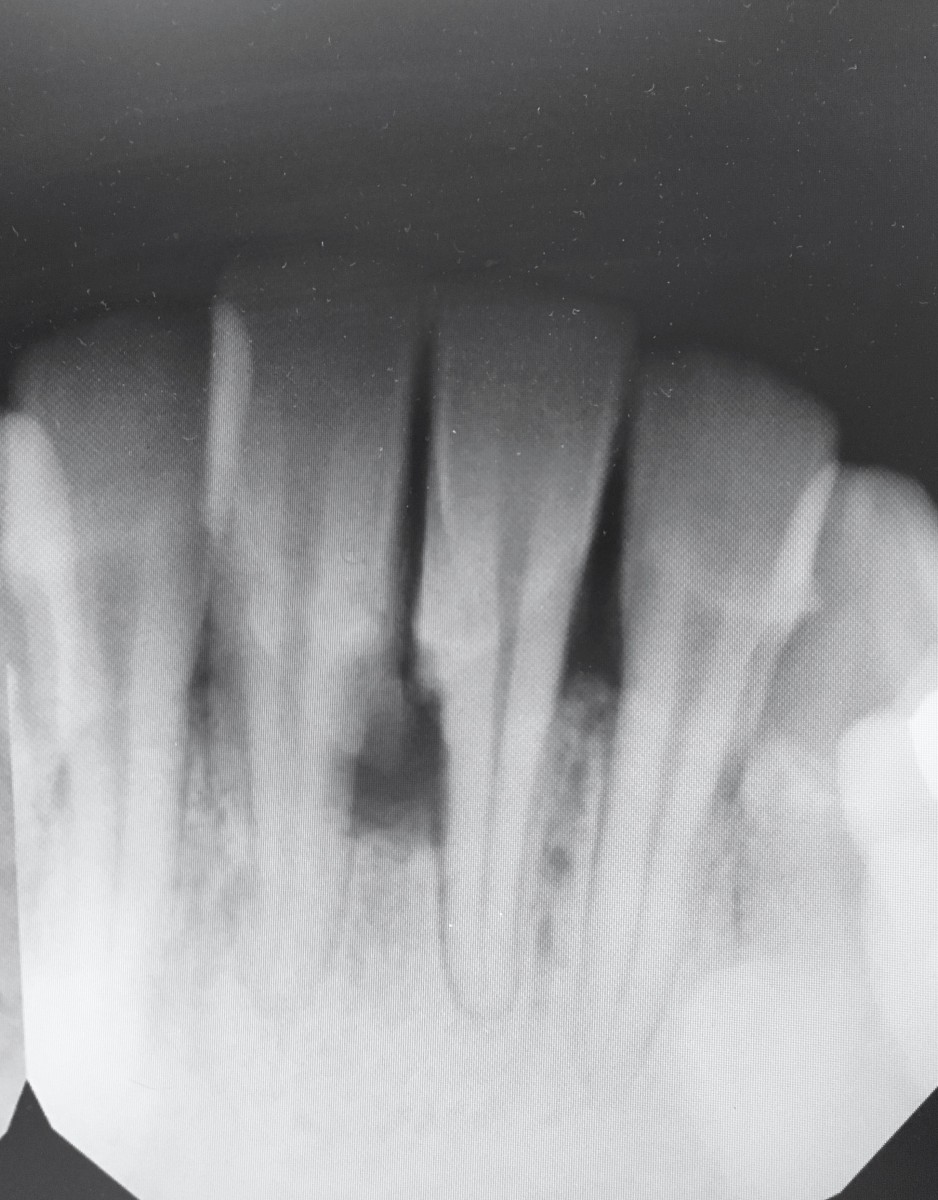
Bone loss that was a concern for mobility.

Lower anterior teeth before the dental prophylaxis.

Buccal and Lingual of lower anterior teeth before treatment.

Lower anterior teeth after scaling. Gingival tissue between teeth #24 and 25 was necrotic.

The lingual view of the lower anterior teeth after scaling. There was only staining left to remove.


