
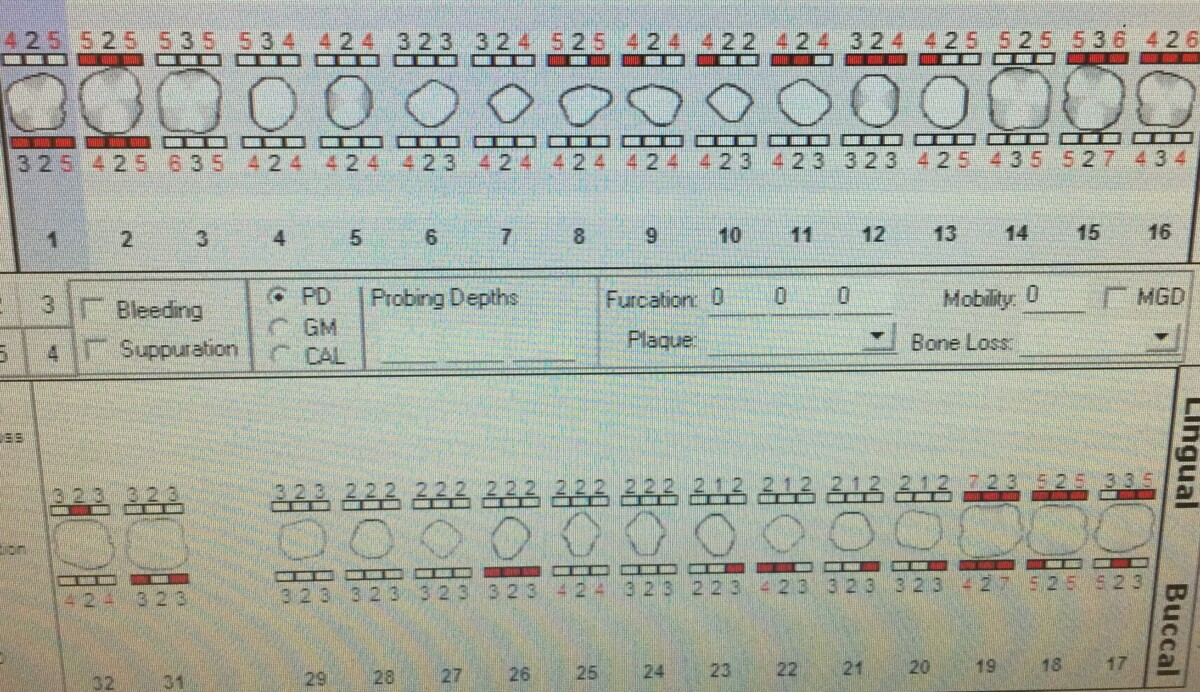
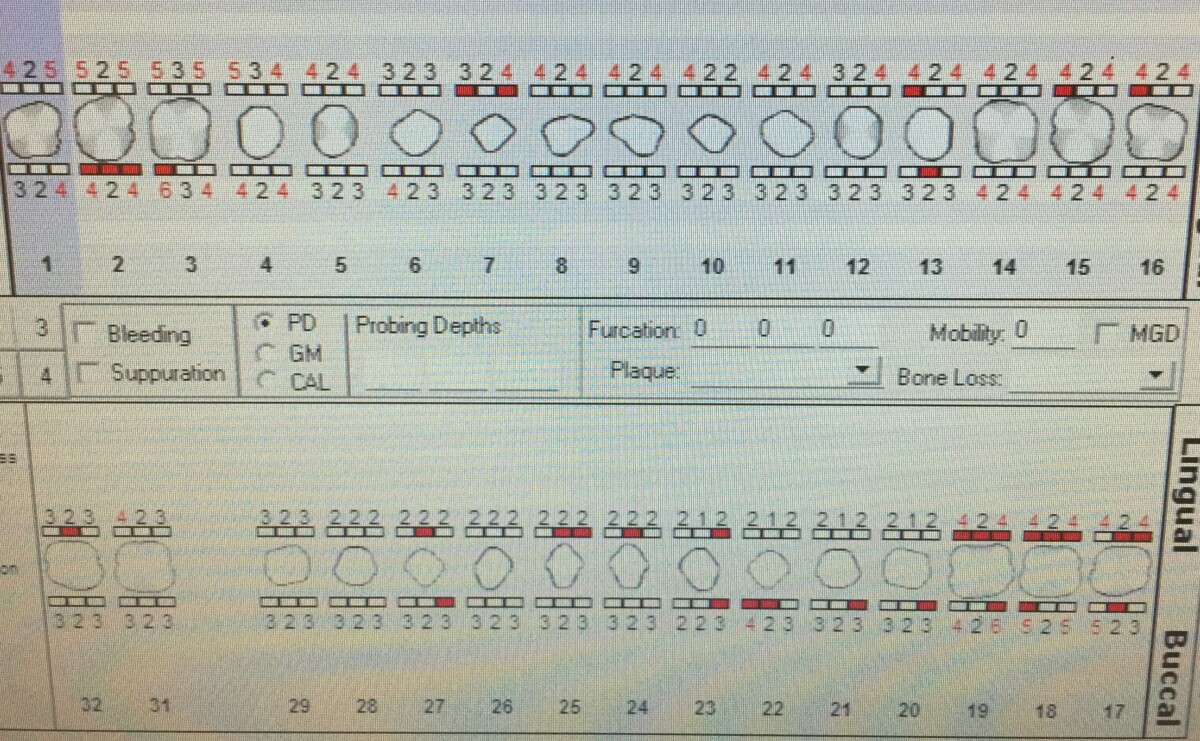
In December 2020, I treated a patient with Arestin. She had Stage II periodontitis with localized moderate bone loss to posterior interproximals on upper left and lower left side. I had my doubts about Arestin’s efficacy at first. This experience, on the other hand, has totally changed my mind. Arestin’s usage makes sense in theory; scaling and root preparation can only go so far in deep pockets. A locally administered antibiotic is a great way to get rid of any remaining harmful microscopic bacteria, especially red-complex bacteria. We were fortunate enough to be offered the chance to try out an expensive treatment help. The patient had localized mild bone loss at first. The four sites where Arestin was given had probing depths ranging from 5-7mm. The patient reported “no discomfort whatsoever” during Arestin placement. The patient returned for re-evaluation in 12 weeks, rather than the 8 weeks we discussed, after allowing the antibiotic to biodegrade. Probing depths were decreased to 4-6mm. Except for one spot that did not shift, the Arestin was clearly effective, as shown by the changes in probing depths. She was diligent in following aftercare instructions, and was very satisfied with the effectiveness of Arestin. However, I believe it would have been easier to administer Arestin immediately after scaling was completed. If not, the gingiva would heal causing it to be firm and harder to apply Arestin. In order to create better access to the sulcus and successfully apply Arestin, I had to lavage the entire mouth to loosen the gingiva and use my instruments to flatten the tips of each cartilage. Therefore, if I were to employ Arestin in the future, I would like to do so on the day scaling was completed if radiographic evidence supports considerable bone loss. Then on the re-evaluation visit, the sites can be examined and engine polished.


{kind=link}
{kind=link}