The patient is a 24 year old Hispanic male. He is ASA II.
The patient’s medical history was reviewed and his last medical check up was in June 2023. The patient reported that he has asthma, smokes marijuana daily and consumes two to three drinks weekly. The ASA classification is II due to further clarification during his medical history interview. The patient mentioned that his asthma attacks were triggered by seasonal allergies, but he has not had an asthma attack since 2020. Therefore, his asthma was deemed well-controlled. I also asked if he still carried an albuterol pump with him. Although he has not used it since 2020, he still keeps it in his backpack wherever he goes. The patient was asked to place his pump chairside in case of an emergency. The blood pressure reading for his initial visit was 134/81 mm Hg which is categorized as stage I hypertension and his pulse was 90 beats per minute. The patient’s last dental hygiene service was in 2019, during which prophylaxis and check up radiographs were completed. His current oral hygiene routine consists of brushing once per day with a medium manual toothbrush. The patient reports difficulty flossing his posterior teeth, so he limits his flossing to only his anterior teeth. The patient uses Listerine mouthwash as needed to freshen his breath. His toothbrush is doubled in function as a tongue brush. The patient also has had orthodontic treatment done from ages 12 to15. There has been no usage of fixed or removable retainers, and some movement of the mandibular anterior teeth has been noted.
Upon examination, the gingiva appears to be pink in color with rolled margins. The mandibular anterior dentition has localized bulbous interdental papilla. The patient has sealants on teeth #12 to #15. Mild attrition has been noted on the anterior teeth. His periodontal charting showed generalized 1-3mm pocket depths and some 4-5mm pocket depths around certain teeth in the mandibular posterior region (see chart). Mild bleeding on probing and plaque accumulation were noted.
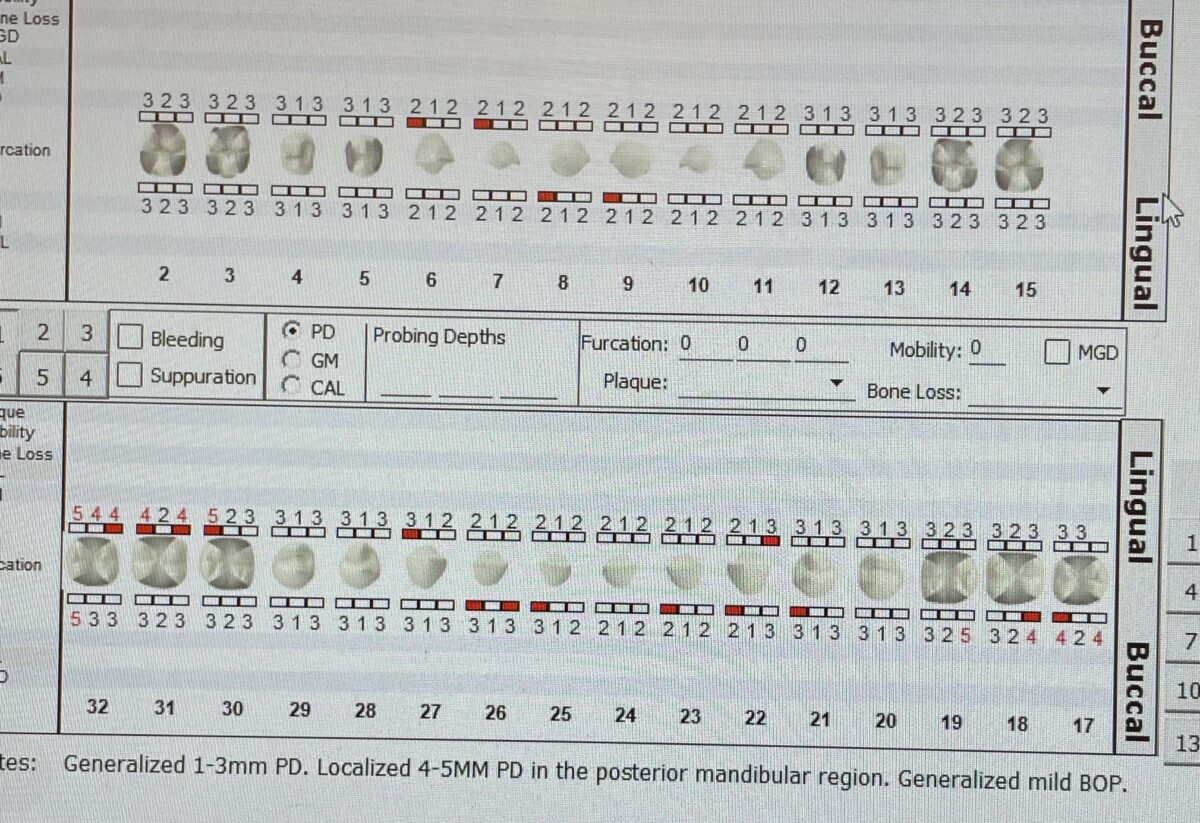
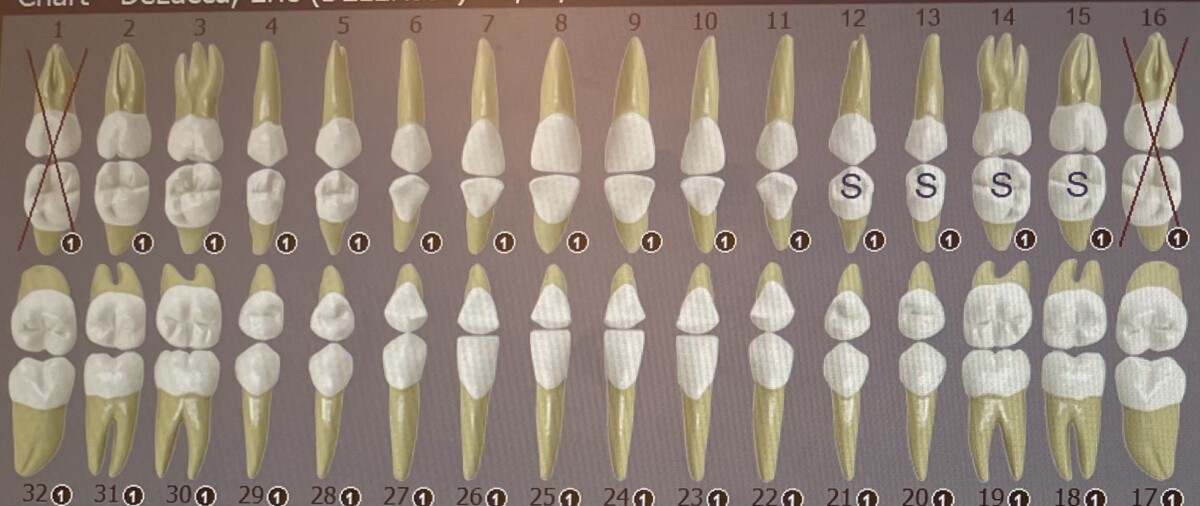
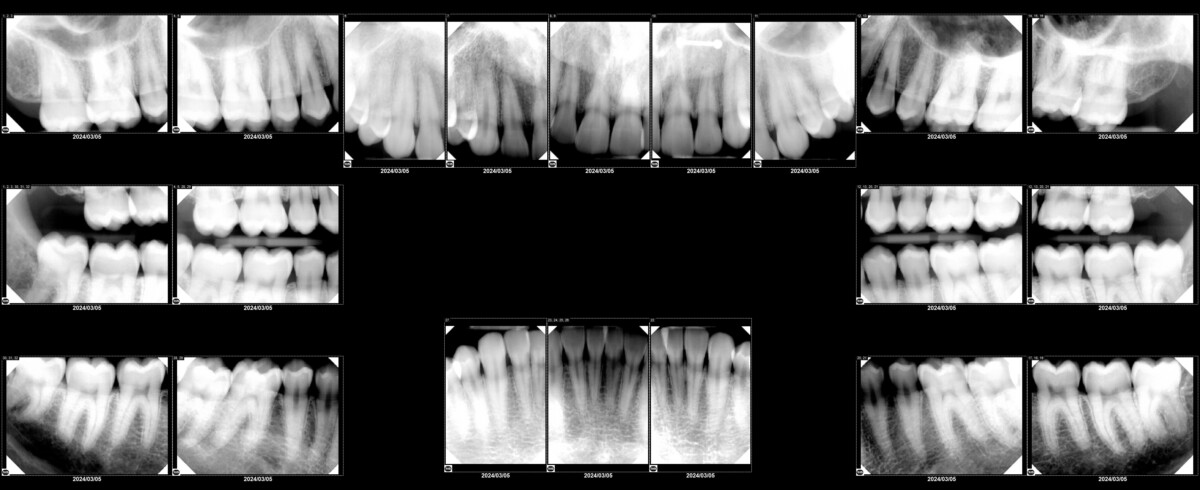
Since the patient reported that his last dental radiographs were taken in 2019 and there were some deeper pocket depths noted on the periodontal chart, I proposed taking a full mouth series of radiographs. Based on the radiographs, no radiographic bone loss or caries were noted. However, generalized radiographic calculus was noted. Using the radiographs, I was able to confirm that the patient’s condition was currently limited to gingivitis. #1 and #16 are congenitally missing.
Using the CAMBRA assessment, the patient was considered moderate risk due to xerostomia as a result of daily usage of marijuana. I recommended the patient to try Biotene mouth rinse to combat xerostomia, xylitol gum to stimulate salivary flow, the use of floss twice per day using the c-shaped flossing method and proper hydration with water. Also, I interviewed the patient to determine if he would like to quit smoking and he was not interested in doing so. I still educated the patient on the increased risk of oral cancer due to his smoking and drinking habit.
Disclosing solution was used prior to scaling and root planing to show the patient where his plaque was to recommend appropriate oral hygiene instructions. Based on the areas where plaque accumulation was noted, we went over the c-shaped flossing technique and I verified that the patient was comfortable with flossing the posterior teeth, as this was a struggle for the patient previously. On a second visit, we reviewed the c-shaped flossing technique again. We also went over the bass brushing method and stressed the importance of brushing twice daily. I thought the patient might need pain management for scaling and root planing since he had a moderate amount of subgingival calculus. However, we decided to try without it and I asked the patient to let me know if he felt any discomfort. He reported no discomfort. After completion of scaling and root planing, I engine-polished and flossed his teeth. A 5% fluoride varnish was applied with aftercare instructions given. Since the patient had gingivitis and did not have an excessive amount of plaque accumulation, I recommended for the patient to come back in six months for his routine cleaning.
A referral was given to the patient for the stage I hypertension reading.

