
MR. J.B.P
Diabetes Type 2
- There are several types of diabetes, but the most common form is Type 2 Diabetes.
- Type 2 Diabetes happens when your body doesn’t use insulin properly
- Insulin is an important hormone produce by the pancreas which helps regulates the amount of glucose in the blood and into the cell, this helps your cells in your body to use the glucose for energy, essential for proper body functioning.
- When this mechanism is impared glucose can’t make its way into the cells and this can lead to both short-term and long-term problems
Sings and symptoms
- Excessive hunger
- thirst
- blurred vision
- fatigue
- Frequent urination
- Slow healing of wounds
- Easily getting infections
Ways to manage it
- Weight loss (Losing at least 7% seems to be ideal)
- Through healthy diets: There is no specific diet but, eating fewer calories, cutting back on refined carbs, specially sweets foods. Adding vegetables and fruits to your diet is essential.
- Exercise: 30- 60 minutes of physical activity every day is recommended
- Medications or insulin
Types of Insulin
- Rapid-acting insulin: begins to work 15 minutes after injection, peaks in about 1 hour, and continues to work for 2 to 4 hours.
- Regular/short-acting insulin: Usually reaches the bloodstream within 30 minutes after injection, peaks anywhere from 2 to 3 hours after injection, and is effective for approximately 3 to 6 hours.
- Intermediate-acting insulin: It reaches your bloodstream about 2 to 4 hours after injection, peaks 4 to 12 hours later, and is effective for about 12 to 18 hours
- Long-acting insulin: Reaches the bloodstream several hours after injection and tends to lower glucose levels fairly evenly over a 24-hour period
Dental Considerations
- Xerostomia
- Dental decay
- Burning sensation
- Impaired/delay wound healing
- Increase incidence and severity of infection
- Secondary infections such as Candidiasis, Parotid gland enlargement, gingivitis and/or Periodontitis
Mr.J.B.P (Periodontitis Stage II Grade B)
New patient
- 33 year old Hispanic. Patient reported having diabetes type 2, last A1C result were 6.7% on January/2021 and currently taking Precose (arcabose) tablets 50mg t.i.d after first bite of every meal.
- Some side effects with this medication can be Diarrhea, gas, upset stomach, constipation or stomach pain, but usually improve over time.
- Last dental visit was on 11/27/20 for a dental prophylaxis and a filling.
- Patient uses manual toothbrush and brush twice a day using a scrubbing motion and Listerine zero alcohol mouthwash every morning.
Intra Oral Findings


- Generalized heavy sub and supra-gingival calculus, patient reported having a dental prophylaxis in Mexico about 2 months ago (Dr. Archer suspected that only ultrasonic debridement was use and that the gingival tissue had shrunk.)
- Gingival statement: Generalized rolled red gingival margins with bulbous papilla with localized cyanotic gingival tissue o the linguals and facials of teeth #7-10.
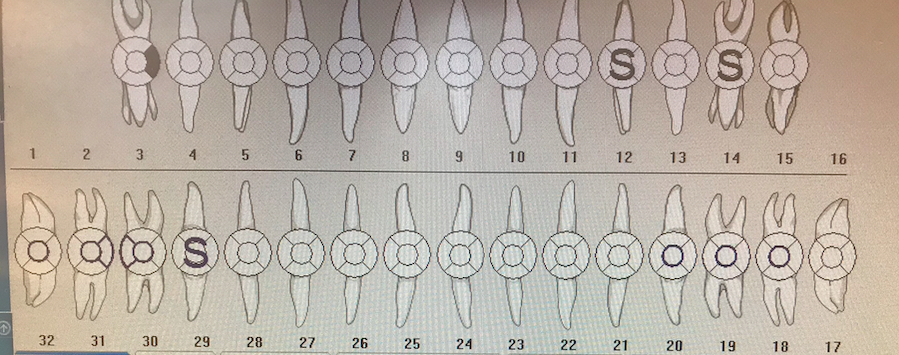
Dental charting
 Patient presented with multiple composite fillings and sealants and decay on tooth #3.
Patient presented with multiple composite fillings and sealants and decay on tooth #3.- Teeth #1, and #16 were not present and tooth #2 was extracted due to caries.
- Caries risk: High with generalized slight attrition.
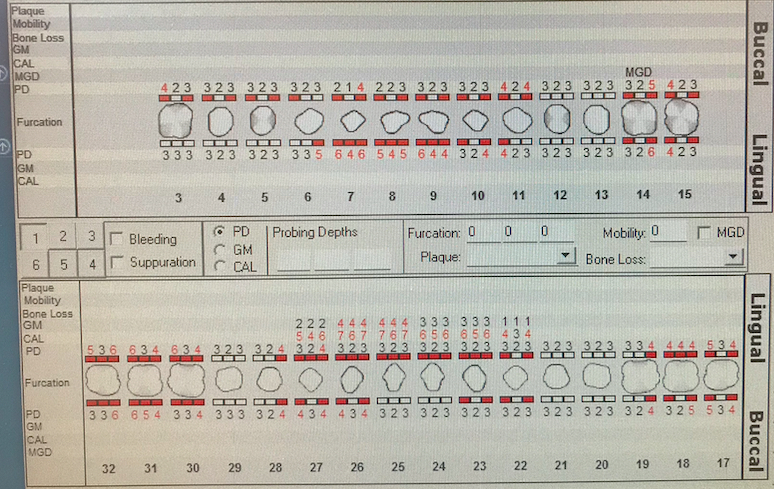
Periodontal Charting
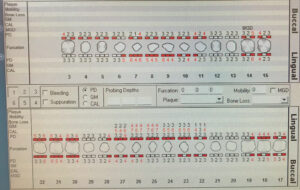 Here we can see severe bleeding upon probing with generalized probing depths reaching 6mm on the posteriors and maxillary anteriors
Here we can see severe bleeding upon probing with generalized probing depths reaching 6mm on the posteriors and maxillary anteriors- Here I recommended FMS dental radiographs for further findings associated with the probing depths and severe bleeding.
Dental Radiographs Findings

- Radiographic caries on teeth #3-M, #4-D(Root caries), Incipient lesion on teeth #18-M, #19-D and #31-M
- We can also see about 30% localized bone loss on teeth #6-9 and on teeth #24 and #25


Treatment Planning and Management!
- Based on the patient medical condition and heavy subgingival calculus, Scaling and root planning were done in 3 visits since people with diabetes tend to heal slower to trauma.
- On the 1st visit I showed the patient the modified bass toothbrush method for proper removal of subgingival biofilm and decided to start scaling sextant 1 and 2 since the maxillary anteriors needed more attention. I did hand scaling with Local anesthesia 2% Lidocaine with 1:100,000 epi on ASA, MSA, PSA, and interpapillary infiltration for patient comfort and to reduce bleeding.
- On the 2nd visit I evaluated the treated areas and notice soft-tissue improvement especially on sextant #2, I reviewed home care and showed the patient how to properly use dental floss, then I scaled the LRQ and sextant #3 to finish treatment on the maxillary. This time I used local anesthesia 2% Lidocaine with 1:100,000 epi on ASA, MSA, PSA, Mental, and Buccal nerve block.
- On the 3rd visit inspected the previously treated areas and major improvement was notice in the gingival appearance, with generalized pink gingival margins with less bulbous papilla and less cyanotic appearance on the linguals of teeth #7-10. I then reviewed homecare and the patient reported having difficulty using traditional floss, so I reviewed with him and also showed him soft picks. Then I hand scaled the remaining quadrant 2% Lidocaine with 1:100,000 epi on the Mental and Buccal nerve block. I then did engine polish due to moderate dental stain and also applied 5% NaF varnish due to high caries risk. An adult referral was also provided for evaluation and restoration for the caries lesions found during assessment.
- For home instructions I recommended brushing twice a day and flossing once a day and for mouth rinses I recommended Listerine antiseptic mouthwash in the morning and ATC fluoride mouth rinse every night to reduce caries risk. A 3 month recall was given.
- Throughout the treatment patient was reminded to take his medications and recommended him to eat before every appointment to prevent any medical emergency.

