Blood pressure is very important for proper body function, but when it’s altered it can cause severe effects on the human body. Hypertension stage II happens when your blood pressure goes above 140 or higher (Systolic) or 90 or higher (Diastolic). This causes an increase in the force of blood pushing against the walls of the veins, arteries, and capillaries, causing damage. In 2018, nearly half a million deaths in the United States included hypertension as a primary or contributing cause.
Over time the force and friction of high blood pressure can cause Heart attack, Heart failure, Stroke, damage to the kidneys, and more. Hypertension stage II, at this stage doctors are more likely to prescribe a combination of medications along with lifestyle changes.
Some examples of prescribe medication can include:
Diuretics: Helps your kidney remove sodium from your body, in return your blood vessels will carry less fluid reducing blood pressure.
Beta-blockers: This makes your heartbeat go at a slower rate and with less force.
ACE Inhibitors: Relaxes your blood vessels, which lower your blood pressure.
Most of this medication may cause oral side effects such as: Xerostomia, Gingival enlargement, Prolong bleeding, and more, affecting the person’s life.
•As Dental Hygienists we play an important role in detecting these conditions since in most cases some patients are not aware they have such condition, since it doesn’t cause any symptoms in most cases.
•With the oral side effects accompanied by their medications we must know how to manage their treatment to improve their everyday life.
•We must be familiar with the signs for an emergency, a good way to remember is F.A.S.T (F: face drooping, A: Arm weakness, S: Speech difficulty and T: Time to call 9-1-1)

W.B., 57 years old Hispanic male. ASA: II. Heavy/Periodontitis stage II/Grade B
Assessment:
•New patient to our clinic.
•He presented with High blood pressure the day of his first visit 134/74. (Revisit BP: 149/69)
•Patient reported his last medical exam was done in February 2015 and reported not having any medical condition. The patient was not aware of having high blood pressure before his visit.
•Last dental visit was April of 2000 for extraction of tooth #3 due to caries
•Patient reported brushing once a day using a scrubbing motion with a manual toothbrush and using Listerine mouthwash once a day. He did not use any interdental aid or tongue cleaner.
•EO Findings: Multiple macules around the face about 1mm in diameter and multiple tissue tags around the neck about 2mm in diameter.
•IO Findings: Missing teeth #1, #3, #16, #17 and #32.
Abfraction on teeth #4, #5, #28 and #29
Attrition on teeth #7,-10 and #21-27
•Initial plaque index was 1.6 (End plaque index :1.0)
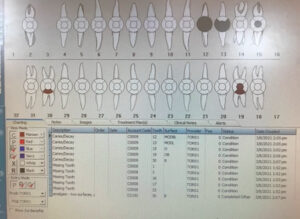

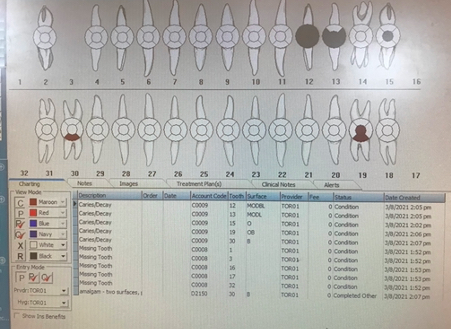
More findings:
On the Upper right image, we can see retain root on tooth #12 and a large cavity on tooth #13 with retained root.
Gingival Statement: Generalized thickened rolled red gingival margins with areas reaching 4mm apical to CEJ and bulbous papilla with severe bleeding on probing.
Left image the URQ was hand scaled and the ULQ was not yet treated, we can see the difference in gingival appearance, on the ULQ looks more rolled margins with bulbous papilla with slight exudate. In contrast, the URQ gingiva seems to be healing with a pinkish in color and fitting snugly around the teeth with slightly pointed papilla.
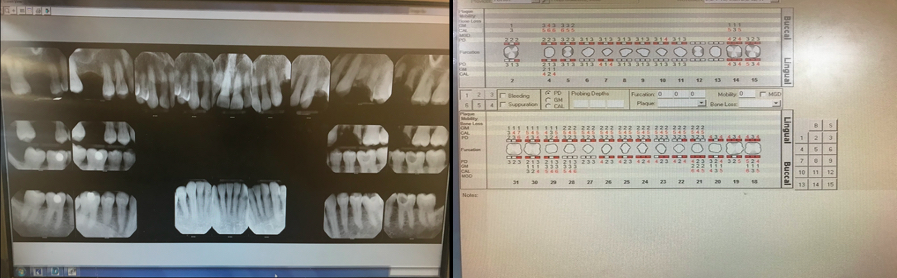
 Periodontal and Radiographic Findings
Periodontal and Radiographic Findings
Here we can see generalized probing depths of 4mm with localized 6mm and clinical attachment loss reaching up to 4mm in some areas.
On the radiographic images we can see missing tooth #3 and the third molars, retained roots on teeth #12 and #13. Generalized 20% bone loss on the maxillary arch and localize 15% bone loss on the mandibular anteriors. Evidence of radiographic calculus and large caries lesion on teeth #18-M and #19-MD
Treatment Planing and Management!
•Based on the patient medical condition and 20 years not having a dental cleaning; scaling and root planning were done in four short visits since the patient could only tolerate one quadrant debridement per visit.
•After each quadrant patient seem very exhausted and asked me to take my time and to give him another appointment.
•All quadrants were hand scaled using local anesthesia (lidocaine 1:100,000 epi)
•Home care instructions: 1st.visit: Modified bass was introduced for subgingival biofilm removal. 2nd.visit: Traditional floss for interproximal cleaning. 3rd.visit: The patient reported having difficulty implementing the flossing technique, so I introduce soft picks (The patient loved it!). 4th.visit: Reviewed everything and recommended the use of Listerine antiseptic mouthwash in the mornings and ACT fluoride mouthwash at nights.
•Engine polish and Fluoride varnish were also provided.
•An adult referral was given for the treatment of retained roots, caries lesions and for a physical evaluation with his primary care provider.
•3 month recall.
With this clinical case, I learned how a medical condition can impact someone’s life, also I learned that some patients do require multiple short or long appointments. Overall, I had an amazing experience with Mr. W.B, I was impressed with how the patient responded after each visit and seeing the healing process of his oral cavity was priceless. Cases like Mr. W.B it’s what keeps me motivated to become a Dental Hygienist!
More After Pictures Enjoy!





 Periodontal and Radiographic Findings
Periodontal and Radiographic Findings

