
Case Study #1 (Stage I Grade A)
23 yr Male
Medical Hx: ASA I, Pt is a non smoker non drinker, Covid tested negative.
Dental: Pt presents with all teeth erupted, no caries visible radiographically or clinically and no restorations.
Moderate Calculus with Heavy Black staining. Low Caries Risk.
Stage I Grade A- Staging and Grading based on radiographic bone loss present and less than 30% present. Periodontal pockets due to loss of bone.
Periodontal charting includes highest pocket depth of 5mm and bleeding present in multiple interproximal areas.
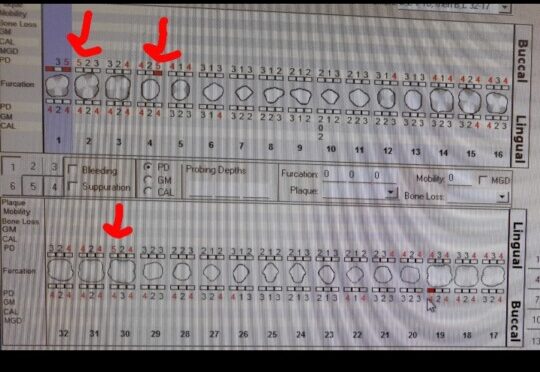
Radiographic statement: Patient exhibits bone loss with a localized molar/incisor pattern. Calculus visible on mesial & distal areas of mandibular incisors and mesial of tooth #30. No caries visible.

Treatment Plan- Patient received plaque index score and first oral hygiene instruction was flossing c shape method technique. It was explained to the patient that this was due to highest probing depth being recorded in interproximal areas indicating proper flossing technique needed to be instructed.
Patient was very compliant and interested in being educated and becoming better at his oral health. Treatment started with the right side to begin debridement in areas needing most care. The patients gingiva responded well to the first treatment and less bleeding was recorded and gum healing was visible throughout visits until completion.
Upon questioning the patient on oral health, it was evident that the black staining was due to heavy tea drinking. Most staining along with calculus was removed by hand scaling using curette instruments. All instruments used for hand scaling included 13/14 gracey, 11/12 gracey and anterior sickle scaler. Staining returned quickly upon patients return and oral hygiene instruction included proper brushing technique 2pid in order to maintain less staining.
With Engine polishing, using a medium grit prophy paste, many of the stains that were still there had completely cleared up and I completed the patients treatment with a 5% NaF varnish to remineralize any areas that have been demineralized.
Case Study #2 (Multiple Supernumerary)
23 yr Male
Pt had no knowledge from previous dental visits of the supernumerary teeth present.
Pt was very pleased with the knowledge I had of radiographs how I was be able to explain his interesting dental anomaly.
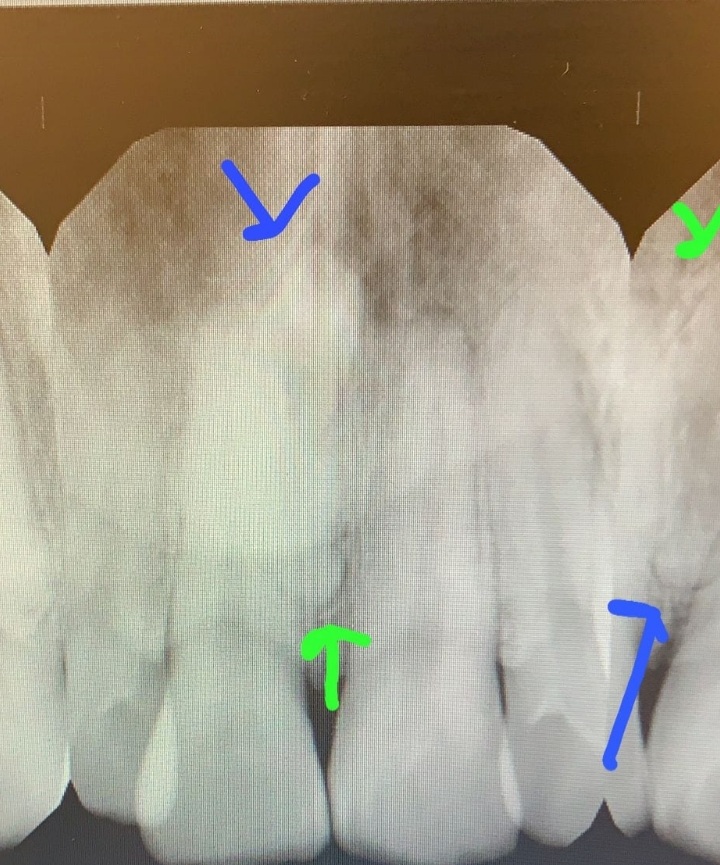
Below there are two supernumerary teeth in the anterior region of the Maxilla, that are radiographically visible.
Supernumerary tooth seen between teeth #8 and #9.
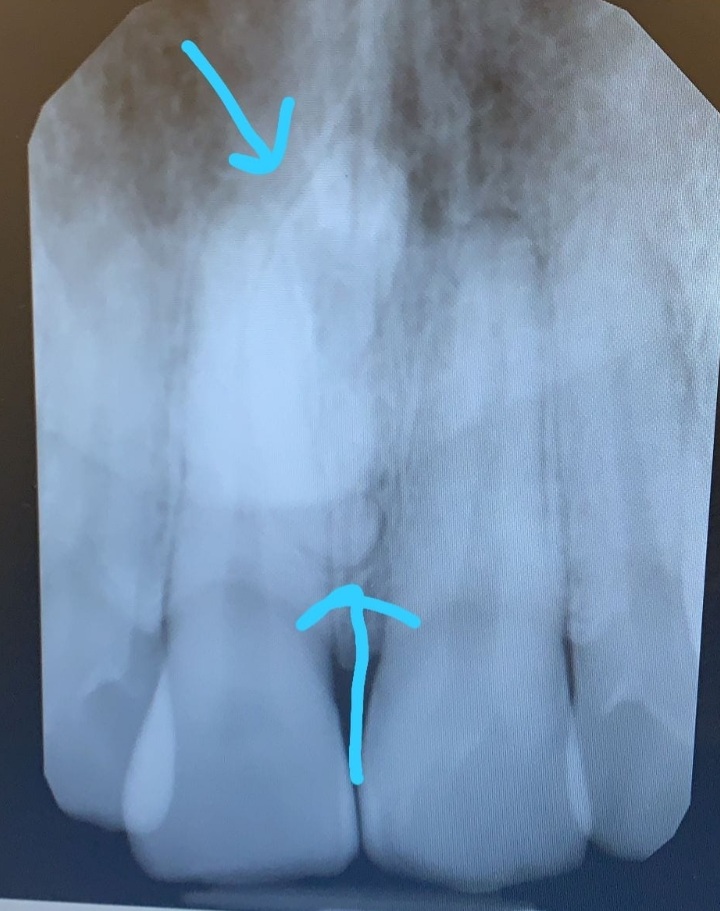
Supernumerary tooth also seen between Tooth# 10 & #11
Case Study #3 (ASA II)
52yr Male ASA II.
B.P 119/88 P:78
Medical Hx: Metropolol 2.5mg 2pid (HBP) Beta blocker, Amlodopine 2.5mg 1pid(HBP) Calcium channel blocker and Esomeprazole 2.5mg 1pid. (G.E.R.D).
Stage II Grade B with Moderate Calculus buildup
Dental Charting: Diastema from teeth #7-10.
Multiple restorations present upon clinical view of patients dentition. Pt.exhibited exocytosis of both maxillary and mandibular facial regions. Bone loss was generalized as 40% and reached a localized 50% in the anterior mandibular region.
Pt presented with gingival hyperplasia due to Amlidopine medication, and xerostomia due to Metropolol and Esomeprazole.
Due to these medications, the patient is considered high risk for caries.

Periodontal Charting: Patient did not exhibit any missing teeth due to periodontitis. Highest pocket recordings of 5mm in multiple areas interproximally.
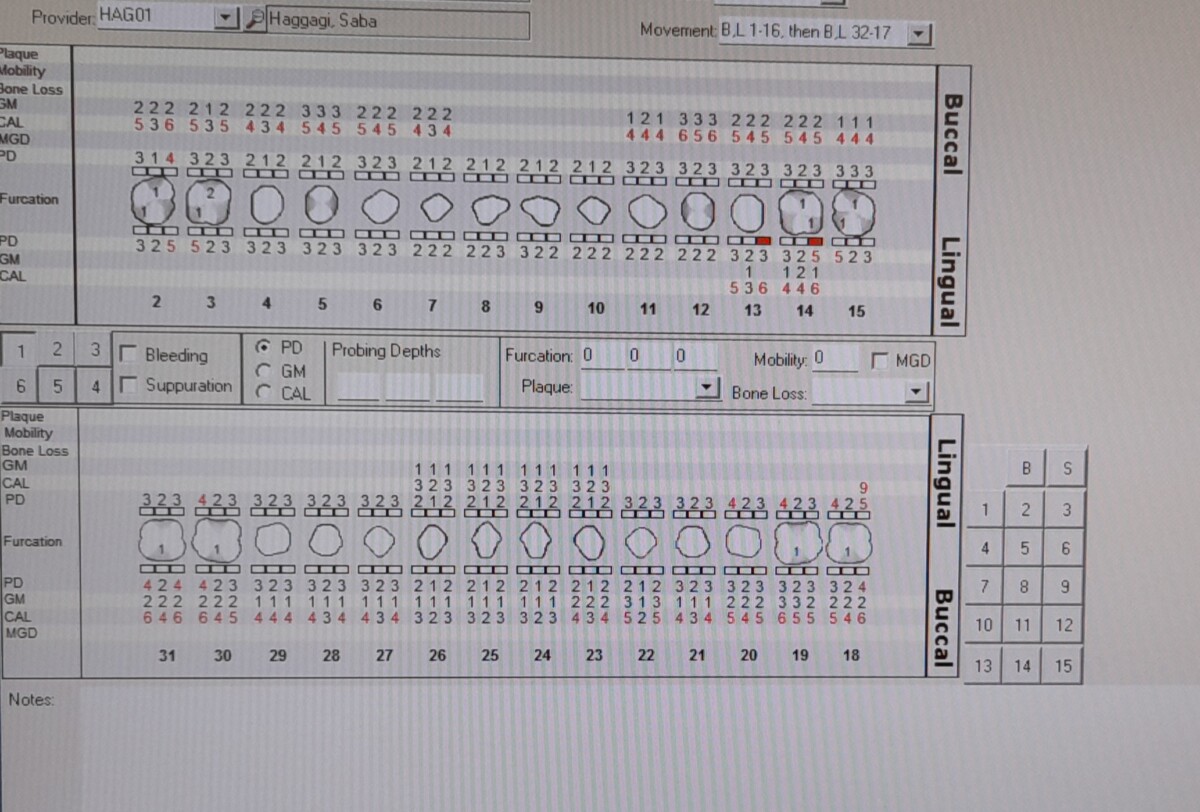
Class 1 furcation generalized in molars facial and lingual aspect with a localized Class 2 furcation on tooth #3L.
Generalized recession of 2-3mm.
Tx Plan: After disclosing patient, oral hygiene instruction of Proxy brushes aid and Listerene Total Care. Pt exhibited type 2 embrasures which indicated a proxy brush was the best choice of interdental aid. Listerene Total Care mouthwash was recommended for caries prevention.
Pt had a mechanical toothbrush in use from previous OHI given.
Completed treatment with the fine prophy paste due to no staining present and use of a 5% NaF varnish in all facial and lingual surfaces presenting with severe recession.
Panoramic view of Exocytosis of the Maxilla and Mandible. Radiographic view shows horizontal bone loss present up to 40% with localized bone loss of 50% in anteriors of mandible.



{kind=link}