Initial Visit
- Recare visit
- 27-year-old African American male
- CC: In need of hygiene services
- Patient reports that he is allergic to penicillin.
- He is also under the care of a cardiologist for hypertension.
- He is prescribed 5mg of amlodipine daily.
- Vitals: 135/90 P: 85, corresponding with stage II hypertension.
- ASA II

Assessments
- Patient has bilateral, palpable, submandibular lymph nodes. Approximately 2mm in size each and asymptomatic.
- Patient presents with a lip ring on the right aspect of his lower lip.
- Bilateral linea alba.
- Exostosis along the mandibular anteriors and the maxillary premolar area.
- Bilateral mandibular tori.
- Bilateral class I occlusion
- 3mm overjet, 95% overbite.

Dental Charting
- Patient is missing #s 1, 16, 17, and 32. He reports that they were extracted.
- #s 5 and 13 are rotated.
- A fracture was observed on incisal edge of #8.

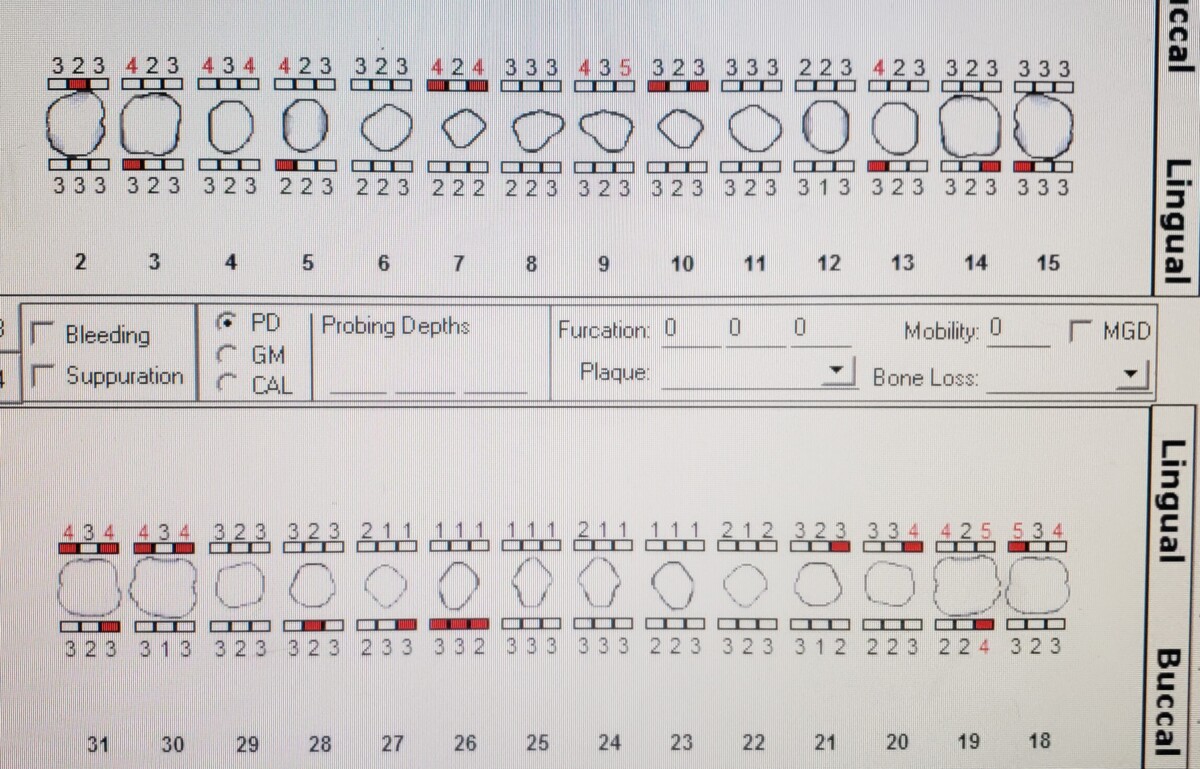
Periodontal Charting
- Patient has generalized probing depths ranging from 1 to 4mm, with a localized area on the left mandibular molars of 5mm.
- There is generalized, mild BOP.
- The gingival margin is coronal to the CEJ, possibly due to his prescribed amlodipine which is known to cause gingival hyperplasia.
Gingival Description
- The gingiva are pink but appear shiny and lack stippling. There is generalized, moderate, marginal inflammation present.
- The gingival margin is coronal to the CEJ, possibly due to his prescribed Calcium Channel Blocker which is known to cause gingival hyperplasia.
- Patient was advised to visit the clinic for hygiene services every 3 months as biofilm and calculus can potentially exacerbate gingival hyperplasia.
About Calcium Channel Blockers
- Calcium channel blockers are a class of anti hypertensive drugs that disrupt the absorption of calcium into the smooth muscles of the heart and arteries.
- Calcium is responsible for the contraction of these muscles and blocking their entry allows the heart rate to slow and the arteries to dilate which in turn lowers blood pressure.
- These medications have the potential to cause xerostomia, orthostatic hypotension, altered sense of taste, and gingival hyperplasia.
Radiographs
- The patient had an FMS exposed in November of 2020 at 7mA and 70 kVp.
- No suspicious lesions were observed.
- Generalized calculus deposited can be seen on the images.
- There is bone lose ranging from approximately 5 to 10%, corresponding with stage 1 periodontitis.

Diagnosis
- Patient has been determined to have stage 1 periodontitis, grade A.
- He has a low caries risk and no active lesions.
- Medium case value due to generalized moderate calculus deposits and well as localized areas of moderate supragingival deposits.
Treatment Plan
- Visit 1: complete assessments, review Bass method of brushing, and hand scale quadrants 1 and 4.
- Visit 2: Review proper flossing method with patient, hand scale quadrants 2 and 3, engine polish with medium grit prophy paste, apply 5% sodium fluoride varnish.
Treatment Plan Implementation
- Visit 1: Completed assessments. PI: 1.3. Reviewed Bass method of brushing with patient. Also recommended Phillips Sonicare electric toothbrush to patient for superior plaque control. Scaled quadrants 1 and 4 to completion.
- Visit 11: Reviewed proper flossing method to patient. Scaled quadrants 2 and 3 to completion. Engine polished with medium grit prophy paste. Applied 5% sodium fluoride varnish and provided after care instructions.
- Next visit in 3 months.

