A 41-year-old Hispanic female (she/her) presented to the clinic for dental cleaning with high blood pressure (Hypertension Stage I). Upon medical history review, the patient reported a history of being overweight, having hypertension, and currently being under the care of a physician. The patient was taking Amlodipine 5mg per os daily but reported her physician discontinued the medication, stating that her blood pressure is now well controlled. The patient also reported that since her last dental cleaning, which was a year prior, she began exercising daily and began to lose weight. I reassured the patient that exercise is crucial for overall health and that she should continue to do so, and to continue with what her physician deems safe.
Upon intraoral examination, a pink, raised, soft tissue lesion about 4mm in size was seen adjacent to tooth 18 on the buccal mucosa. Also, tissue trauma/sloughing was seen on the mucosa opposing teeth 27-29. The patient was informed of the findings and stated she was aware of both lesion and tissue sloughing, and that the lesion did not cause her any pain. Dr. Brown, a specialist at NYCCT dental clinic, was shown the lesion and determined it to be a fibroma.

The gingival assessment revealed mild inflammation localized to the lower lingual surfaces with red and rolled margins. The dental assessment revealed abrasions on teeth 5 and 6, indicating the patient may be using too much pressure while brushing this area.
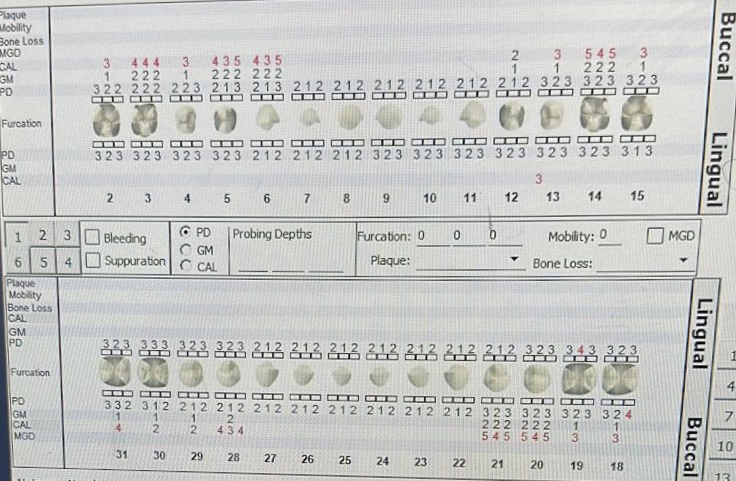
The periodontal assessment revealed 1-3mm probing depths with localized 4mm probing depths and CAL on all buccal surfaces of posterior teeth. Radiographs were indicated. After assessments were complete, I determined her to be a light case value. I developed a treatment plan with 1 visit to expose a PAN and 4 horizontal bite wings, review power toothbrushing, scale the entire mouth and apply 5% fluoride varnish.


Four horizontal bitewings and a Panoramic radiograph were taken. Some vertical and horizontal bone loss was seen on the bitewings. Unerupted tooth 1, mesioangular impacted tooth 16 and a radiopacity distal to the apices of tooth 18 were seen radiographically. The patient was informed of all findings and given a copy of the radiographs. Based on all data collected clinically and radiographically, the patient’s periodontal status was determined to be Stage I Grade A Periodontitis, with a low caries risk.
I proceeded to disclose the patient. A Plaque Index score of 0.8, with plaque mainly along the cervical third, illustrated the patient needed to improve on their power toothbrushing technique. Therefore, for oral hygiene instructionI reviewed the amount of pressure the patient should use while brushing due to the recession present, as well as angling the power toothbrush at a 45-degree angle in order to clean under the gumline. Furthermore, I briefly spoke to the patient about switching to an alcohol-free mouth rinse to help with the tissue sloughing. The patient understood. After, prophylaxis was performed and completed, and the patient was dismissed with a referral to see an oral surgeon for possible removal of the impacted tooth 16. The patient was pleased with the level of care I provided in a timely manner and vowed to leave a great review in the patient survey.

