
-
Recent Posts
Recent Comments
Archives
Categories
Meta
Ayurveda and Traditional Chinese Medicine: A Comparative Overview
Posted in Uncategorized
Leave a comment
Our Tour of the Rubin Museum of Art

Image from the Rubin Museum website. Click for source.
Our customized private tour of the Rubin Museum of Art is scheduled for 11:00 AM next Wednesday morning, December 11. The museum is at 150 W. 17th Street (between 6th and 7th Avenues) in Manhattan. Our tour will last approximately one hour.
Photos of most objects are permitted and there is a restaurant on site if you are up for lunch afterwards (sadly the grant cannot treat us to eats though). Let me know if you have any questions!
Posted in Uncategorized
2 Comments
What is Harm Reduction?
Please go the the International Harm Reduction Association’s website at www.ihra.net and read, “What is Harm Reduction? A position statement from the International Harm Reduction Association.” After doing so, watch the International Drugs & Harm Reduction Film Festival 2013 winner for best film: ‘The Journey of Change.’ (see www.ihra.net/film-festival)
Ask yourself the following when watching the film, and post comments:
1) What is the journey of change?
2) What are the specific risks and harms associated with drug use?
3) What causes those risks and harms?
4) What can be done to reduce these risks and harms?
5) Does the view of drugs in the film represent a view of harm reduction or even, the way we view drug use in the US? Think about the songs we played for you, how they took a light-hearted, perhaps cryptic, rousing, comical or dark view of addiction.
6) What emotions did the short film illicit? What would you want to take away from it?
Thanks,
Aida & Gwen
Posted in Uncategorized
Leave a comment
Honoring a Physician in an Opera
I was going to post this example of commemorating a physician in an opera after Dr. Bert Hansen’s excellent talk on how Life Magazine honored members of the medical profession via photography, but this post also fits in with our examination of songs.
In any case, a while ago we were privileged to attend a performance of an opera-in-progress entitled “Semmelweis” at the New York Academy of Medicine. The composers of the opera, Ray Lustig (music) and Matt Gray (words) are writing the opera under the auspices of the Brooklyn-based American Opera Projects and they have chosen a terribly sad story to tell.
If you are like me, you’ve never heard of Ignaz Semmelweis, but he certainly deserves to known and esteemed for his ground-breaking work that was never honored (and actually sneered at) during his lifetime.
Ignaz Semmelweiss. Image from Wikipedia, click for source.
Semmelweis was born in 1818 in Hungary to German Jewish parents. He graduated from medical school in Vienna in 1844 and became an obstretrician at a prestigious teaching hospital there.
There were two maternity clinics at the hospital. At that time, many women died after childbirh from puerperal (“childbed”) fever. Women who gave birth in Clinic One were attended by physicians and medical students and women who gave birth in Clinic Two were attended by midwives and their students. Semmelweis noticed that the mortality rate for women in Clinic One was very much higher than the mortality rate in Clinic Two, In fact, women who gave birth outside in the street had a lower mortality rate than the women who delivered with the help of the doctors.
The discrepancy bothered Semmelweis and he began keeping statistics on all sorts of factors in an attempt to discover the reason why more women were dying in Clinic One. The only difference he could find was that the doctors and medical students would go directly from conducting autopsies to delivering babies without washing their hands.
No one knew from germs back then but Semmelweis conjectured that there was something about the cadavers that was causing the childbed fevers. He believed “cadaverous particles” that he could smell were causing the deaths.
So, Semmelweis instituted a new policy that required attending physicians to wash their hands with bleach before they delivered babies and sure enough, the mortality rate in Clinic One dropped by 90% .
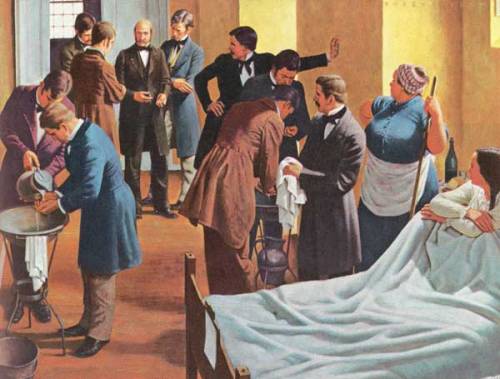
Semmelweiss making doctors wash their hands. Click for source.
Sadly, many doctors disagreed with Semmelweis’ theory and ignored or even ridiculed him. Part of their problem was that they refused to believe their highly educated hands could carry anything harmful and part of their disdain was because they just didn’t like Semmelweis who wasn’t sophisticated – he was a Jewish foreignor who spoke with an accent and so they discounted his ideas.
By 1850 the hospital effectively forced him out and Semmelweis moved to Budapest where he took a much less prestigious job at a hospital there. He reduced the really high rate of childbed fever there to less than 1% of birhs. Still, most doctors refused to wash their freaking hands.
Semmelweis became depressed and obsessed with reducing the rate of childbed deaths. He wrote some Open Letters to prominent European obstreticians in which he essentially accused them of murdering women with their irresponsible behavior. Semmelweis was rightly peeved but his behavior became erratic. He was drinking and staying away from his family and when he turned 47, a colleague lured him to an insane asylum and had him locked up. Poor Semmelweis tried to escape and the guards beat him so badly that he died of an infection two weeks later.
Of course, years later, Louis Pasteur’s work vindicated Semmelweis. Today there are hospitals named in his honor in Austria and Hungary. Germany honored him in a 1956 postage stamp:

Click for source. Depositphotos.
There is even a psychological reaction called the “Semmelweis Reflex” which Wikipedia defines as “a metaphor for a certain type of human behavior characterized by reflex-like rejection of new knowledge because it contradicts entrenched norms, beliefs, or paradigms”.
After we enjoyed the wonderful opera (and to be honest I’m not usually a fan of the genre), some physicians in the audience talked about the dismal maternal mortality rates in modern day New York City. Maternal mortality rates here are 30% higher in 2013 than they were ten years ago and the racial disparities here are shocking, Only three states in the US have worse maternal mortality rates than New York. Semmeweiss would be rightfully horrified.
Posted in Uncategorized
Leave a comment
Addiction and Harm Reduction Recap

Dynamic graphic by the Austin Harm Reduction Coalition
As promised, I’m uploading Gwen’s and Aida’s mp3’s from last week’s session on addiction and harm reduction, aptly titled “Addiction, Illness, Death, Dying and Redemption.” The songs are too big to be uploaded onto the OpenLab, so I’ve added links to the songs (most are videos):
The Eagles, Life in the Fast Lane
Dr. Hook and the Medicine Show, Penicillin Penny
Ben Folds, The Secret Life of Morgan Davis
Ben Folds and Nick Hornby, Picture Window
Neil Young, The Needle and The Damage Done (with some nice personal intro)
And here’s my contribution to the addiction-theme songs: Jane’s Addiction, Jane Says
Following our discussion of these songs, I did a quick search on the concept of harm reduction, which seems a logical practice to address addiction. I was surprised to learn that it seems to be a relatively new strategy from the late-twentieth century and there’s resistance to its implementation. I found an article by a G. Alan Marlatt, “Harm Reduction: Come As You Are,” Addictive Behaviors 21, 6 (1996): 779–788 that seems to summarize the harm reduction approach. I’m not sure how fundamental his work is to the field but he provides a good overview, plus I like his title, which seems appropriate following our music session since it also alludes to a Nirvana song. Another relevant article is Bernadette Pauly’s “Shifting moral values to enhance access to health care: Harm reduction as a context for ethical nursing practice,” International Journal of Drug Policy, 19, 3 (2008): 195–204 that highlights the disconnect of implementing strategies of harm reduction and real-world healthcare practice, and the larger question of ethics for practicing nurses. I’ve included the abstracts below.
Marlatt Abstract:
The purpose of this paper is to describe what harm reduction is, how it developed, how it works, and why it is becoming a major approach in the addictive behaviors field. Based on principles of public health, harm reduction offers a pragmatic yet compassionate set of strategies designed to reduce the harmful consequences of addictive behavior for both drug consumers and the communities in which they live. To illustrate how harm reduction has been applied to both the prevention and treatment of addiction problems, highlights of a national conference on harm reduction are presented. The historical roots of harm reduction programs in Europe (Netherlands and the United Kingdom) are described. The paper concludes with a discussion of four basic assumptions central to harm reduction: (a) harm reduction is a public health alternative to the moral/criminal and disease models of drug use and addiction; (b) it recognizes abstinence as an ideal outcome but accepts alternatives that reduce harm; (c) it has emerged primarily as a “bottom-up” approach based on addict advocacy, rather than a “topdown” policy established by addiction professionals; and (d) it promotes low threshold access to services as an alternative to traditional high threshold approaches.
Click here for PDF of Marlatt article
Pauly Abstract:
Background
People who are street involved including those experiencing homelessness and substance use are at increased risk of morbidity and mortality. Such inequities are exacerbated when those facing the greatest inequities in health have the least access to health care. These concerns have rarely been addressed in bioethics and there has been a lack of explicit attention to the dominant societal and organizational values that structure such injustices. The purpose of this paper is to describe the underlying value tensions that impact ethical nursing practice and affect equity in access to health care for those who are street involved.
Methods
In this paper, findings from a larger qualitative ethnographic study of ethical practice in nursing in the context of homelessness and substance use are reported. The original research was undertaken in two ‘inner city’ health care centres and one emergency department (ED) to gain a better understanding of ethical nursing practice within health care interactions. Data were collected over a period of 10 months through face-to-face interviews and participant observation.
Results
In order to facilitate access to health care for those who are street-involved nurses had to navigate a series of value tensions. These value tensions included shifting from an ideology of fixing to reducing harm; stigma to moral worth; and personal responsibility to enhancing decision-making capacity. A context of harm reduction provided a basis for the development of relationships and shifted the moral orientation to reducing harm as a primary moral principle in which the worth of individuals and the development of their capacity for decision-making was fostered.
Conclusions
Implementation of a harm reduction philosophy in acute care settings has the potential to enhance access to health care for people who are street involved. However, explicit attention to defining the harms and values associated with harm reduction is needed. While nurses adopted values consistent with harm reduction and recognized constraints on personal responsibility, there was little attention to action on the social determinants of health such as housing. The individual and collective role of professional nurses in addressing the harms associated with drug use and homelessness requires additional examination.
Click here for PDF of Pauly article
Reminder: Shauna Vey’s Talk tomorrow Nov 14
Just a friendly reminder that one of our team members, Professor Shauna Vey will be giving a talk tomorrow Thursday, November 14, on her research on nineteenth-century child actors in Atrium 631 at 1:oo pm.
Posted in Announcements
Leave a comment
Interdisciplinary Course Proposal
I found the form for proposing a new interdisciplinary course on the College Council website under the Curriculum Committee’s Major Modifications button. It is daunting.
I am working on my portion of the Weekly Course Outline (3-5 weeks depending on what we decide) on the right to die, patient autonomy, living wills, dnr orders and health care proxies, as well as how various cultures mourn and commemorate their decedents through the fine arts (incorporating a trip to a museum, case law, a film(?) and a novel).
Here is the form:
New York City College of Technology, CUNY
NEW COURSE PROPOSAL FORM
This form is used for all new course proposals. Attach this to the Curriculum Modification Proposal Form and submit as one package as per instructions. Use one New Course Proposal Form for each new course.
| Course Title | |
| Proposal Date | |
| Proposer’s Name | |
| Course Number | |
| Course Credits, Hours | |
| Course Pre / Co-Requisites | |
| Catalog Course Description |
|
| Brief Rationale
Provide a concise summary of why this course is important to the department, school or college. |
|
| Intent to Submit as Common Core
If this course is intended to fulfill one of the requirements in the common core, then indicate which area. |
|
| Intent to Submit as An Interdisciplinary Course | |
| Intent to Submit as a Writing Intensive Course |
Please include all appropriate documentation as indicated in the NEW COURSE PROPOSAL Combine all information into a single document that is included in the Curriculum Modification Form.
NEW COURSE PROPOSAL CHECK LIST
Use this checklist to ensure that all required documentation has been included. You may wish to use this checklist as a table of contents within the new course proposal.
| Completed NEW COURSE PROPOSAL FORM |
|
|
|
|
|
| Completed Library Resources and Information Literacy Form |
|
| Course Outline
Include within the outline the following. |
|
| Hours and Credits for Lecture and Labs
If hours exceed mandated Carnegie Hours, then rationale for this |
|
| Prerequisites/Co- requisites |
|
| Detailed Course Description |
|
Course Specific Learning Outcome and Assessment Tables
|
|
| Example Weekly Course outline |
|
| Grade Policy and Procedure |
|
| Recommended Instructional Materials (Textbooks, lab supplies, etc) |
|
| Library resources and bibliography |
|
| Course Need Assessment.
Describe the need for this course. Include in your statement the following information. |
|
| Target Students who will take this course. Which programs or departments, and how many anticipated?
Documentation of student views (if applicable, e.g. non-required elective). |
|
| Projected headcounts (fall/spring and day/evening) for each new or modified course. |
|
| If additional physical resources are required (new space, modifications, equipment), description of these requirements. If applicable, Memo or email from the VP for Finance and Administration with written comments regarding additional and/or new facilities, renovations or construction. |
|
| Where does this course overlap with other courses, both within and outside of the department? |
|
| Does the Department currently have full time faculty qualified to teach this course? If not, then what plans are there to cover this? |
|
| If needs assessment states that this course is required by an accrediting body, then provide documentation indicating that need. |
|
| Course Design
Describe how this course is designed. |
|
| Course Context (e.g. required, elective, capstone) |
|
| Course Structure: how the course will be offered (e.g. lecture, seminar, tutorial, fieldtrip)? |
|
| Anticipated pedagogical strategies and instructional design (e.g. Group Work, Case Study, Team Project, Lecture) |
|
| How does this course support Programmatic Learning Outcomes? |
|
| Is this course designed to be partially or fully online? If so, describe how this benefits students and/or program. |
|
| Additional Forms for Specific Course Categories |
|
| Interdisciplinary Form (if applicable) (under development) |
|
| Common Core (Liberal Arts) Intent to Submit (if applicable) |
|
| Writing Intensive Form if course is intended to be a WIC (under development) |
|
| If course originated as an experimental course, then results of evaluation plan as developed with director of assessment. |
|
| (Additional materials for Curricular Experiments) |
|
| Plan and process for evaluation developed in consultation with the director of assessment. (Contact Director of Assessment for more information). |
|
| Established Timeline for Curricular Experiment |
|
Posted in Uncategorized
Leave a comment
Series on Medical Burnout in the NYT

Ansel Adams, Nurse Hamaguchi presents a baby to her mother, Manzanar Relocation Center CA, 1943
Just a quick note to tell you that NYT writer David Bornstein has been writing about burnout in healthcare, and the different ways health professionals have been seeking meaning in their work. His latest commentary “Who Will Heal the Doctors” was published Oct 2nd, 2013. Bornstein’s series is rather doctor-centric but as I read it, I couldn’t help but think how many of the issues he brings up is pertinent to all who work in the healthcare field. In this latest article, Bornstein mentions a course called The Healer’s Art that helps students and doctors reconnect to the deeper meanings of their work. I looked at The Healer’s Art website and they have courses geared to work with all healthcare professionals. You can look at their program for nurses here. Off the website, the course covers topics including “deep listening, presence, acceptance, loss, grief, healing, relationship, courage, lineage and self-care practices.” We have spent a lot of time on the importance of observation and the need for careful looking. I was glad to see the importance given to listening, in particular deep listening, a form of communication that our students should be trained in to promote greater empathy with their patients.
UNM article
Edited UNM Submission I posted the abstract and article we submitted to UNM
I will post the sildes next week when I’m done with them
Posted in Uncategorized
Leave a comment

