My patient Ms. C was a 21-year-old Asian female who presented for a regular dental checkup. Her vitals were 115/76 with a Pulse of 66. She is ASA2 due to the mango allergy reaction. The patient’s last dental examination and dental cleaning was in 2014, and she had never had any dental radiographs taken. The patient brushes twice a day with a Philips electronic toothbrush but rarely uses any interdental aids.
Bilateral linea alba and lip piercing at the midline of the lower lip below the vermillion border were documented during the extraoral and intraoral examination.
The patient has a Class I occlusion with a 5mm overjet and a 50% overbite. The mesial of tooth #18 was chipped. Tooth #17 and #32 were impacted.
The patient had generalized heavy marginal gingival inflammation as well as BOP. Her gingiva was red in color, smooth and shiny, puffy in consistency, and bulbous interdental papilla. The gingiva of maxillary and mandibular anterior areas were flaccid. Except for the posterior molars that had a localized 5mm PD, the pocket depths were generalized ranging between 2-3mm. During the calculus detection process, generalized heavy supragingival and subgingival calculus was identified. The calculus was black in color.
A treatment plan was developed and discussed with the patient. FMS digital radiographs, whole mouth scaling with oraqix or local anesthesia for pain management, and 5% sodium fluoride varnish application were all planned.
During the initial visit, FMS was exposed using 7mA and 70kV. The patient’s FMS revealed that she had 10% generalized horizontal bone loss and generalized calculus was shown on the interproximal. Suspicious caries presented on #3DO, #4MOD, #5DO, #14DO, #19MO, and #20DO.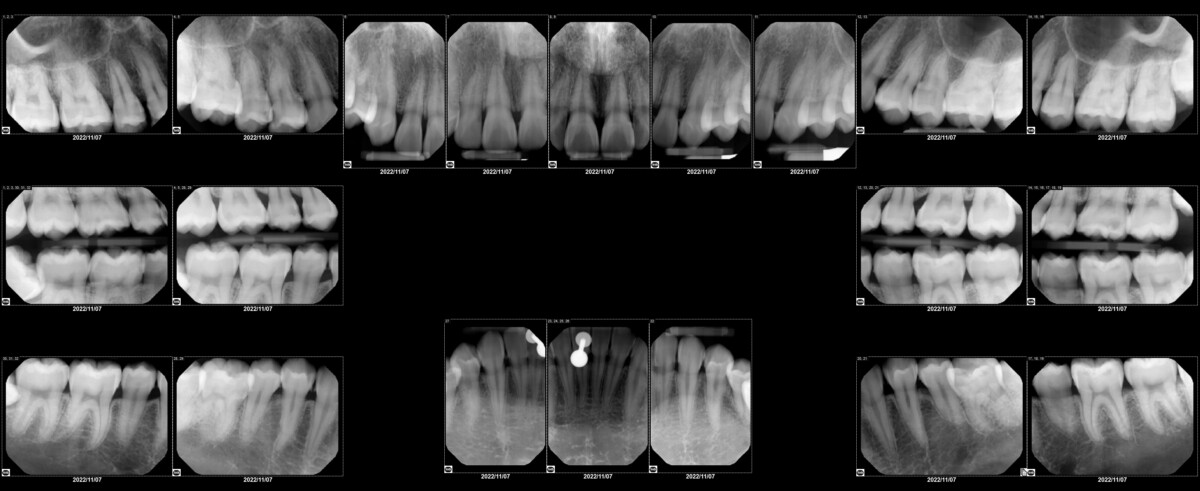
Her plaque index score was 1.2, which is considered fair. Biofilms were found primarily on the cervical third and interproximal. The patient was demonstrated how to brush with a powered toothbrush and floss. Suggested the patient remove her lip piercing to prevent further mucogingival defects. The patient reported that she could practice properly on her own. She noticed an improvement in her oral health after implementing the OHI and had removed her lip piercing when she came back for 3 months recall.
The patient’s full mouth scaling treatment was completed with the use of ultrasonic scalars and hand instruments. During the initial visit, the dentist administered 72 mg lidocaine with 0.036 mg epinephrine LA. The patient tolerated the procedure well. On the patient’s request, Oraqix was used during the second appointment instead of LA. 5% sodium fluoride varnish was applied after the completion of scaling. The patient was given a copy of the FMS and a referral for caries evaluation.
Her gingival soft tissue responded favorably. When she returned for her three-month recall appointment, she appeared to have less inflammation and BOP. The patient was pleased and complied with the OHI very well.
Before Treatment
After Treatment

