This is a very special case for me since she was one of my first patients that I had the pleasure to treat and see every 3 months. I got an excellent opportunity to learn about other conditions and how they affect our mouth and body.
Oral Interview
This case will present a 71-year-old African American female with a history of high blood pressure, kidney transplant in 2019, type 2 diabetes with the most recent HbA1c value of 6.1, glaucoma, asthma, blood transfusion, GE reflux, osteoporosis, and sleep apnea—everything well controlled. ASA 3
Medications:
- tacrolimus 0.5 mg 2x a day
- Tretinoin 0.05% cream to face
- clobetasol propionate ointment usp 0.05 2 x a day
- Duloxetine 20 mg
- Ozempic 4 mg/3ml
- Mycophenolate 500 mg
- Latanoprost ophthalmic solution 0.005
- Triamcinolone 0.1 lotion 3x a week
- Vitamin D 10 mcg 2x a day
- Vitamin B 2x a day
- Albuterol inhaler 2 puffs as needed
The patient is not drinking or smoking.
She complains of a dry mouth. Previously, she was brushing two times a day with a manual toothbrush, Crest toothpaste, and Listerine alcohol rinse at night. She is not using her sleep apnea machine, flossing, or using a water flosser. She goes for regular dental cleanings and checkups every 6 months.
Assessments
EO: 5×5 mm brown elevated regular-shaped mole located on the chin; patient reports having that checked by a dermatologist every year.
IO: Biting marks on the lateral side of the tongue.
Dental Charting: Overbite 40%, Overjet 5mm, Occlusion Class I on the right side, and Class II on the left side.
Gingival Statement: The gingiva was generalized pigmented with areas of pink, with localized mild red, inflamed, soft, and smooth gingival margin on the lingual side on the maxillary and mandibular arch by the premolar and molar areas. Localized mild bulbous on maxillary facial anterior teeth.
Periodontal Charting: Generalized 1- 4 mm pockets with localized 5 and 6 mm on posterior teeth. Generalized recessions of up to 2 mm. Furcation involvement class 2 on tooth #30.
PI score: 1.2 (fair)
CAMBRA: moderate due to patient medications that cause xerostomia,
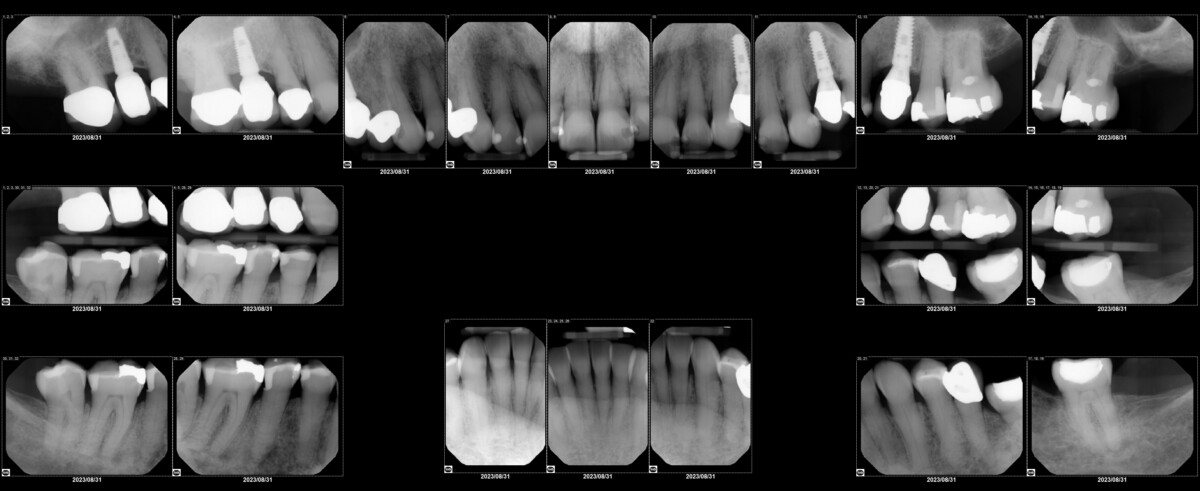
Radiographic Statement: Using 7 mA and 70 kV FMS, 20 images were taken. There were no suspicious caries, no calculus present, no suspicious lesions, and no impacted teeth. Generalized horizontal and localized vertical bone loss of up to 20%. The patient is missing teeth #1, 2, 14, 15, 16, 17, 19, and 32.
Implementation
She was classified as having localized medium periodontitis, stage III, grade B. Based on the assessments, a treatment plan was developed. There were three appointments to compensate the patient.
Initial visit: medical history was taken, all assessments completed, PI score, treatment plan signed, and dental radiograph completed.
1st revisit: Quadrants 1 and 4 scaled to completion, with Topical 20% Benzocaine Gel.
2nd revisit: re-evaluate quadrants 1 and 4 and scale quadrants 2 and 3 to completion with topical 20% benzocaine gel. Engine polished and applied 5% Sodium Fluoride Varnish.
OHI: electric toothbrush with soft bristles twice a day; flossing with regular string floss at night; biotene mouthwash for xerostomia due to patient medications; recommended to start using a sleep apnea machine.
Evaluation
The patient is now on a 3-month recall. The patient was very compliant with OHI. After instructions were given, she started to brush twice a day with an electric toothbrush and floss with string floss at night. The patient changed her oral rinse to Biotene mouthwash to minimize xerostomia. As I had pressure to see her every 3 months, the patient now has light periodontitis, stage III, grade B, with very good oral hygiene. The PI score went down to 0.5, and her dry mouth is not as severe as it was before. The gingival margins are mild dark pink and firm.

