Type II Diabetes, Hypertension, Hyperlipidemia, and Hypothyroidism
Recare Visit:
CC: “Dental Cleaning”
Demographic: 64 y/o Asian female, Blood Pressure: 118/78, Pulse: 72.
Medical History: Last physician visit: 12/2023. Last HbA1c: 6.4 (12/2023). Patient does not report any new medications and reports taking medications as prescribed. Patient is currently taking medications to manage type 2 diabetes, hypertension, hyperlipidemia, and is taking Levothyroxine post thyroidectomy in 2013. No adverse side effects reported. Pt reports eating prior to appt.
Current medications: Metformin 500mg 3x/day, Januvia 50mg 1x/day, Benicar 40mg 1x/day, Lipitor 10mg, 1x/day, Levothyroxine 75mcg 1x/day.
ASA 2 due to controlled hypertension and type II diabetes.
Dental History: Last dental visit: 12/12/2023 for arestin check. Last dental x-rays: 3/10/2023 (4VBWs). Patient reports using a Philips Sonicare electric toothbrush 2x/day. Patient reports using string floss and a water flosser 1x/day, Listerine Total Care and a tongue scraper 2x/day.
Clinical Examination:
EO/IO: Right TMJ clicking, palatal torus, coated tongue. Exostoses on buccal maxillary premolar and molar area and on facial mandibular incisor area.
Dental Charting: 4mm overjet, 70% overbite. Abfraction on #7. Class 1B furcation on #30. MID fracture on #24 and MI fracture on #25. Class 1 mobility on #23-26. Generalized moderate attrition.
Gingival Statement: Gingiva is generalized pink with marginalized redness. Gingiva is rolled, blunted, spongy, smooth, and shiny. Mandibular lingual gingiva is moderately red compared to maxillary lingual gingiva. Generalized posterior buccal recession 1-3mm. Embrasure class 2. Gingival margin is 1-2mm coronal to the CEJ. Light bleeding upon gentle exploring.
This clinical presentation suggests continued inflammation, indicating a persistent inflammatory host response within the periodontium.
Periodontal Charting: Generalized 2-3mm with localized 4-5mm and 1-3mm recession in the posterior region. Light BOP.
-
- Calculus: Generalized supragingival deposits and localized subgingival deposits. Case value: Medium, Stain: Heavy generalized staining and occlusal and buccal pit staining.
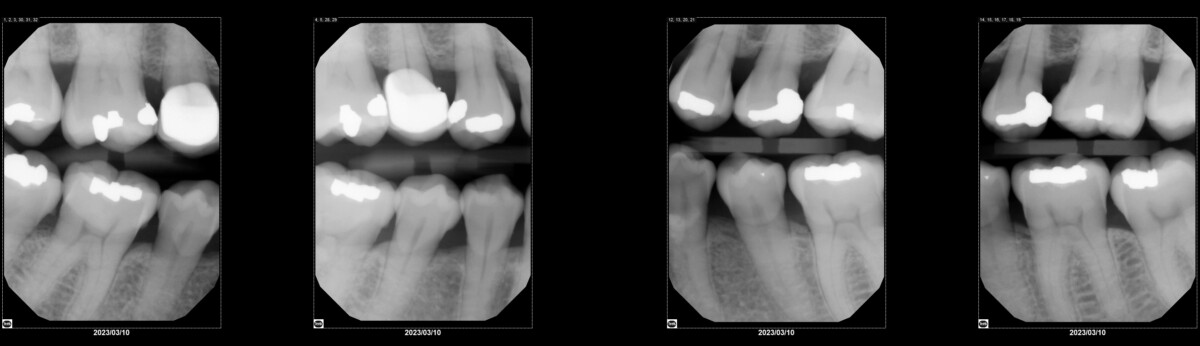
- Radiographic statement (from 03/2023): Generalized 15% horizontal RBL. Localized 5-10% vertical RBL between teeth #’s: 5-6, 12-14, 28-30. Calculus present on teeth #’s 14, 15, 30, 31. No radiographic caries present. Patient informed of all findings.
- Periodontal Status: Stage 2 Grade B
- Caries Risk: Moderate
- PI Score: 1.17- interproximal, marginal, and on tongue
Reviewed medical and dental history, all assessments completed: EO/IO, dental charting, periodontal charting, calculus detection. CAMBRA: Continue oral hygiene routine, recommended patient to consume coffee and tea using a straw to minimize staining, to consume all carbonated beverages primarily during mealtimes, and recommended Act anticavity mouthrinse. OHI: Reviewed and demonstrated the electric toothbrush to minimize marginal plaque. Patient demonstrates understanding. Completed scaling Q1 and Q4 using ultrasonic and hand scaling.
Revisit #1:
Reviewed medical and dental history: patient reports being able to use her electric toothbrush as instructed every night. OHI: reviewed and demonstrated c-shaped string floss for the anterior teeth and interdental brushes in areas with class 2 embrasure spaces to effectively remove interproximal plaque. Patient demonstrates understanding. Completed scaling Q2 and Q3 using ultrasonic and hand scaling. Engine polished with coarse paste, flossed all contacts, and applied 5% fluoride varnish. Post-op instructions given.
Recare: 3 months
To provide comprehensive care and maintain bone levels to prevent further progression of periodontal disease, all aspects were considered including medical and dental history during all recare and revisit appointments. This patient has been under my care for routine 3 month SRPs since her initial visit on 03/06/2023. Initially she presented with very heavy tenacious black subgingival and supragingival deposits and she was previously only brushing her teeth with a manual toothbrush as part of her oral hygiene routine. Since her initial visit until now, there have been drastic improvements in not only her calculus build up, but also her own oral hygiene routine. The importance of not only brushing, but also using various interdental aids such as a water flosser, interdental brushes, as well as mouthrinse specific to her case are necessary to control biofilm and minimize prolonged inflammatory response of the body.
This patient qualified for 4 arestin sites which were placed in September 2023 and checked in December 2023. Although probing depths remained the same, we noticed the sites where the arestin was placed were no longer bleeding when probed.
Because the patient also presents with controlled type 2 diabetes, hypertension, and hyperlipidemia, it is important to reiterate the importance of visiting her primary care physician on a regular basis to ensure all necessary bloodwork and lab exams continue to remain within normal limits. By addressing the patient’s medical and dental history in conjunction with frequent recalls and nonsurgical periodontal therapy, we can effectively manage their periodontal disease, prevent further progression, and maintain current bone levels.
Radiographs from 3/10/2023: