
Patient profile:
• Ms KN is 22 years old female.
• Patient currently lives in Brooklyn, New York. She is single, no children. Moved to USA couple
years ago, has bachelor degree in accounting, planning to applying to college again, but currently
works in a restaurant as a waitress. Patient doesn’t have any medical or dental insurance, has to pay
for each visit or treatment out of pocket.
• Ms KN has an Eastern-European background, and was raised with belief that it is not important to
see the dentist unless something bothers you.
• Last dental exam was in August 2018. One Full Mouth Series were taken. Last and first dental
cleaning was done in May 2017.
• KN reports to brush 2 times a day using soft manual toothbrush using a back and forth motions,
prefer Colgate whitening dentifrice, flosses once in a while, using Chlorhexidine once a day for the
last month due to her gingiva condition.



Chief Complains
• Patient states that: “My gingiva is getting enlarged, I saw two doctors, but they could not tell
me the reason why. It does not look nice and painful sometimes. My gums almost always bleed
when I brush my teeth. “
• Patient presented with localized red, raised gingiva adjacent to maxillary left central and lateral
incisor. Generalized moderate gingival inflammation.
• Ms KN would like to have her teeth cleaned so she would not feel embarrassed anymore and it
would not interfere with her daily life.
Health History Overview
• Blood Pressure on initial visit 106/73, Pulse 90, ASA I
• Patient presented with oral pyogenic granuloma.
• Patient is in a overall good health, non smoker, non drinker, no allergies to food or medications.
• Ms KN reports not taking any prescribed or over-the-counter medications, supplements or herbs.
Explanation of Condition
• Pyogenic granuloma is a reactive hyperplasia of connective tissue in response to trauma, local irritants
like calculus accumulations, overhang restorations, poor oral hygiene, hormonal changes or
medications.
• Common signs: tumor like, soft, vascular, nodular growth in the oral cavity. Color can be purple pink
or red, depending on vascularity, can become fibrotic with a time. Histologically it appears as
exuberant granulation tissue. Does not appear radiographically. Children and females are more
frequently affected due to hormones. Despite the fact that its called granuloma, it doesn’t contain any
pus. This condition is benign.
How Condition is managed
Treatment of pyogenic granuloma depends on the origin. If it is associated with poor oral hygiene and
calculus accumulations, full mouth debridement is necessary prior any treatments. Pregnancy relates, most
of the time it decreases in size after pregnancy.
– Curettage and cauterization: Pyogenic granuloma is scraped off and blood supply are being cauterized.
– Laser surgery removal: will remove and burn the lesion.
– Surgical removal: very small reoccurrence, but requires sutures.
Dental Hygiene Management
• There are no contraindications for dental hygiene treatment. In case with Pyogenic granuloma, oral
health is critical.
• Due to high vascularity origin of the lesion, bleeding is the primary complication during treatment.
• If calculus is identified as the main cause, adjacent teeth must be scaled to prevent recurrence.
• Bleeding or ulceration of the pyogenic granuloma can be cause of development of secondary
infection.
• Most people are feeling concern due to cosmetic reasons.
Summary of Clinical Findings
- EO: No significant
- IO: -maxillary attached gingiva, adjacent to the teeth #9 and 10, well demarcated, red, soft,15mmX8mmX2.5mm elevated lesions suspect pyogenic
- – Labial mandibular mucosa, adjacent to teeth # 23-27, white plaque appears from the
- Occlusion: Class I, Overjet 3mm, Overbite 25%
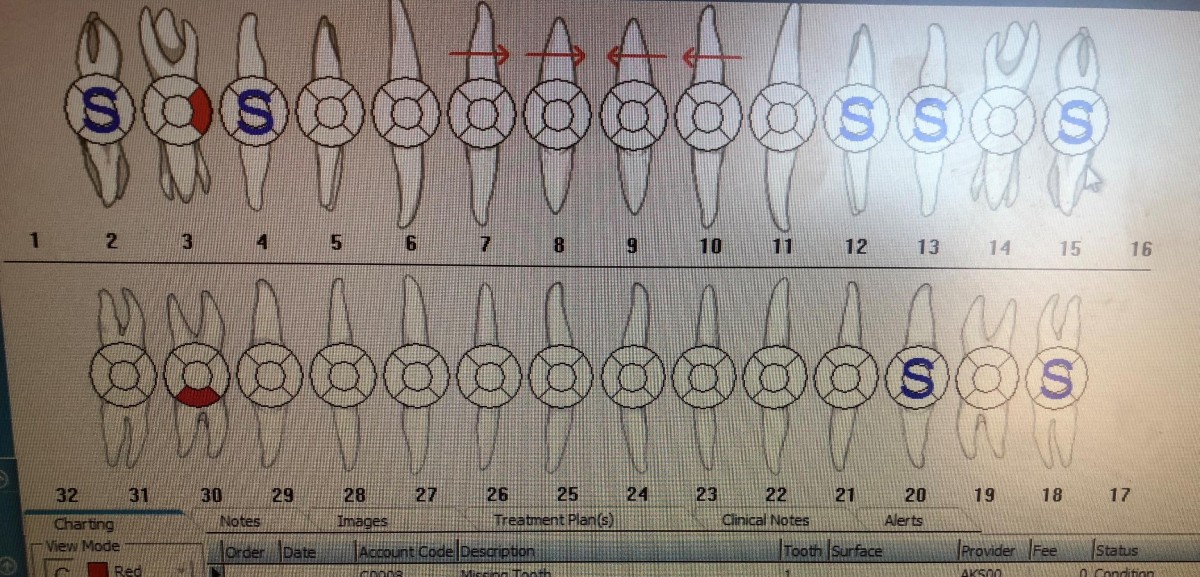
- Dental: Class I composite restoration on occlusal of #29.
- -Sealants present on #2, #4, #12, #13, #15, #18, #20, #31.
- – Suspicious caries lesion on #3M, #30B
- – Diastema between #7, #8, #9, #10.
Deposits: Heavy calculus present mostly on posterior teeth
- Generalized plaque noted mostly on cervical third of the teeth
- No extrinsic stains were noted
Gingival Description & Periodontal Status
- Gingiva: generalized pink, well contoured, stippled gingiva, fits snuggle around the posterior teeth, moderate inflammation. Localized bulbous, red, raised interdental papillae and attached gingiva adjacent to teeth #9,10. Localized red, rolled gingival margins on the facial and lingual anterior teeth of the mandible, #22-27.
- Generalized active Perio/Type 1 (Gingivitis)
- Generalized BOP
- No bone loss evident (without radiographs)
- No attachment loss
- No recession is evident
- No mobility
Dental Hygiene Diagnosis
- Generalized active Perio/Type1 Gingivitis due to:
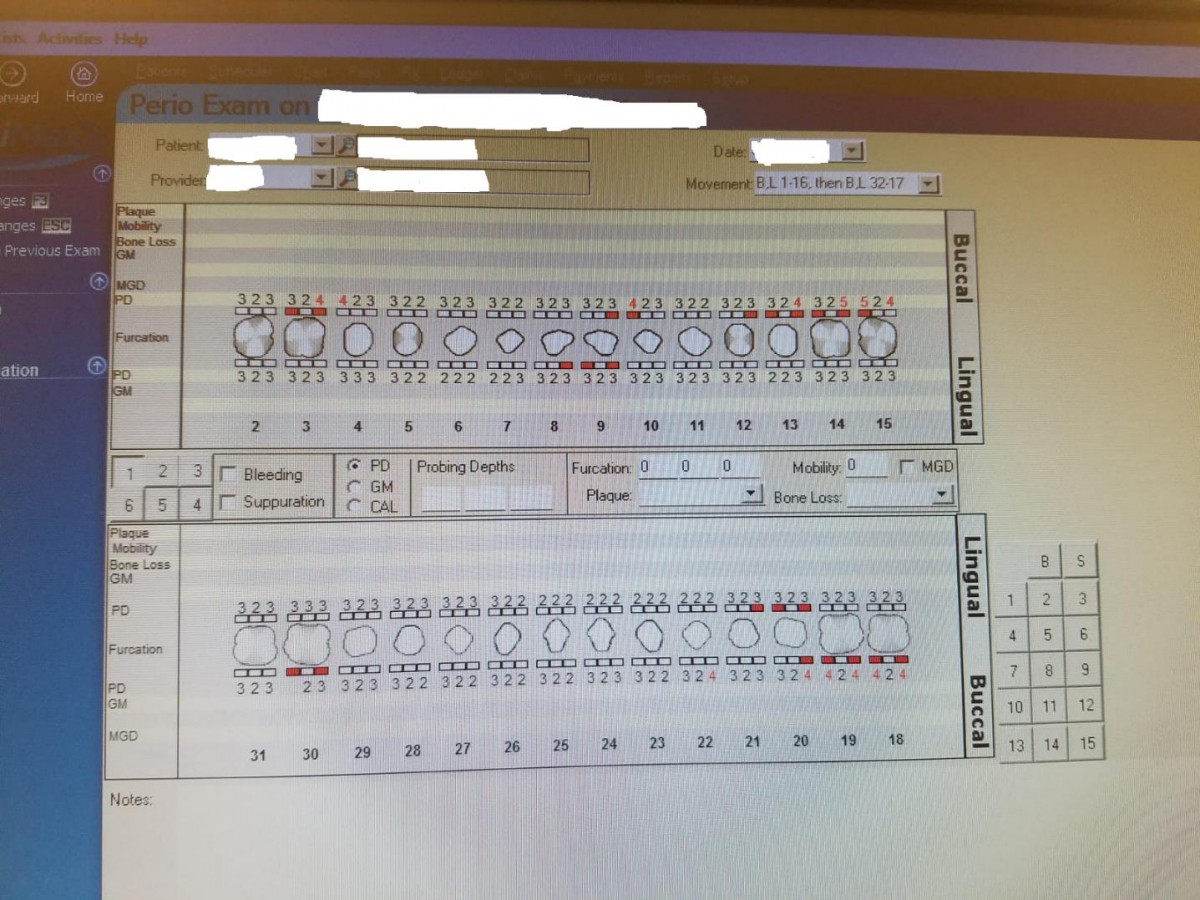
- generalized 2-3mm probing depths, localized 4-5 on posterior teeth (#3M, #4D, #10M, #13D, #14D, #16M,#16D, #18M, #18D, #19D, #19M, #2OD, #22D
- moderate BOP,
- no evidence of bone loss due to not having radiographs available
- caries Assessments risk: According to the ADA Caries Assesments risk patients consider to be at moderate risk due to 2 suspicious caries lesions in the last 36 months, no dental home established.
Dental Hygiene Care Plan
- Eliminate BOP in 50% by 6 MRC.
- Reduce plaque index to 0.6 to by 6 MRC.
- Patient will be reporting using waxed floss as interdental aid 3 times a week by 6 MRC.
- Patient will reporting using Modified Bass Tooth Brushing Method using soft manual toothbrush by 6 MRC.
- Patient will be reporting using Antiseptic Oral Rinse with fluoride once a day for 30 seconds by the 6 MRC.
- Patient will be reporting using night guard during the night by the 6 MRC.
- Patient will report establishing dental home by 6 MRC.
Treatment Implementation
- Oral Self-Care instructions: patient was taught the Modified Bass Tooth Brushing method using soft manual bristled tooth brush. Particularly for the area with Pyogenic granuloma, patient was advised to use tuft end tooth brush to keep the area free of biofilm. In addition, the proper flossing technique using loop method was shown for interdental aid. Tongue cleaner was introduced for removing residual debris, patient was advised to use it three times a
- Fluoride Therapist: Ms. KN was advised to switch the toothpaste to 1.1% sodium fluoride containing dentifrice. Upon patient completion, 5% sodium fluoride varnish was
- Sealants: Patient already had sealants
- Antimicrobial: Patient was advised to use Antiseptic Oral Rinse Listerine (Original or Cool Mint Brands were given as examples) twice a day for 30 seconds using swish
- Dietary Guidelines: Patient was recommended to increase fruits and vegetables.
- Debridement Performed: Debridement was completed using FSI-power 1000 triple band ultrasonic and hand instruments as anterior sickle scaler, greyces 1/2, 11/12, 13/14, posterior nevi scaler, universal curet. There was severe bleeding on where there were soft tissue inflammation, which was stopped by applying constant pressure with gauze. Patient had major sensitivity in this area, which was managed with applying non- injectable local anesthesia “Oraqix” (2.5% lidocaine and prilocaine periodontal gel).
- Engine polished was performed using fine paste to remove residual plaque and smooth the
Upon completion, patient received 5% sodium fluoride varnish application due to caries prevention.
- During debridement patient was well managed. Patient responded well to pain management. The main difficulty during debridement was difficulties in removing the tenacious sugvingival calculus


Continued Care Recommendations
- Patient was recommended for 6 MRC
- Continue using Oral B powered tooth brush 2 X a day, tuft end toothbrush was advised for localized tissue inflammation.
- Use Listerine waxed floss 3 X a week
- Antiseptic Mouth wash 1 X a day for 30 seconds
- 5 % NaF varnish application at 6 MRC
- Night guard
Positive final reflection
During the treatment patient was compliant with a home care instructions. She was very interesting in learning about periodontal disease process and how it impacts on overall health. Ms.KN noticed significant reduce in bleeding during tooth brushing. In addition to that, she was very pleased in significant decrease in size of pyogenic granuloma
- I felt strong with patient communication. Last semester I did not feel comfortable with talking to patients and giving recommendations about new products.
- It was very good experience to work on a patient with tenacious deposits. I was able to identify my weak spots that have to be improved.
Critical final reflection
- My treatment plan had to be modified adding two extra appointments to complete the patient due to tenacious calculus deposits
- During the assessment part, I wasn’t able to recognize the pyogenic granuloma due to lack of oral pathology knowledge on that moment. My instructor informed my patient about condition and what causes
- During the dental charting, I confused sealants with composite restorations. I knew rationale for sealants, but since I haven’t seen that in clinic yet, I though it was a new kind of restoration I was not aware
- During oral hygiene instructions, instead of showing Modified Bass tooth brushing method, I felt I should have recommended Powered tooth brush form the beginning. Patient showed interest in obtaining one later. I did not want to overwhelm the patient with so many oral hygiene strategies, that was the main reason why I did not introduced patient interproximal brush for maxillary incisors.
- During the debridement phase of the treatment, it took me a significant amount of time to remove the deposits. I did not know how to use the ultrasonic scaler properly: I didn’t apply lateral pressure to the deposit. Neither the length of the stroke was adjusted no the boost mode was used. When working with hand instruments, I felt that my hands was not powerful enough to apply enough lateral
- I was so engaged with removing the deposits, that did not realize that my ergonomic positions were poor. Having back pain form after the clinic session emphasize the impact of poor dental.

