Case Study #2: Managing Patient With Medical Conditions
Patient Profile
- Mr.R. is an 81 year old caucasian male.
- Patient currently takes Lipitor (Atorvastatin) 250mg/ Once a day for high Cholesterol levels
- Patient also takes Diuril (Chlorothiazide) 125 mg for Hypertension for the past 4 years.
- Patient is a medium case value/ Perio stage 2 grade B.
- Patient uses electrical toothbrush and flosses twice a day, uses a waterpik
- Patient does not use Oral rinses.
Chief Complaint
- Patient was mainly concerned about getting a dental cleaning .
Health History Overview
- Blood Pressure: 135/76 Pulse:79. It was elevated, we asked if took his medication that day and stated he has. He was aware and was told to keep seeing his doctor for his hypertension.
- ASA II
- Current health conditions: Hypertension and cholesterol.
Hypertension
Hypertension is the term to describe high blood pressure, it is the measurement of the force exerted against the walls of your arteries as your heart pumps blood to your body. Elevated blood pressure exceeding 130 over 80 mmHg is known as hypertension.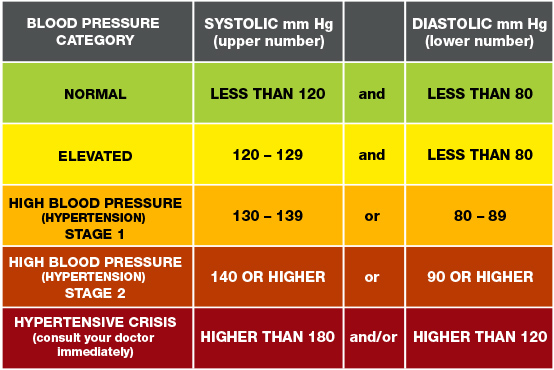
Hypertension increases the risk of various adverse cardiovascular events such as atherosclerosis, stroke, coronary heart disease and other serious life threats.
Hypertension In The Oral Cavity
- Periodontitis and hypertension have common risk factors, smoking, stress, increased age, and socioeconomic factors.
- There is a correlation between high blood pressure values in individuals with missing teeth, tooth extraction and tooth loss among adult’s factors that contribute to periodontal disease
- Patients having hypertension and severe periodontitis have a correlation of chronic inflammation where bacterial plaque destroys the epithelium of the periodontal pocket and breaks the barrier that isolates the tissue and circulation, allowing the entry of harmful elements in the bloodstream
Dental Complications With Hypertension
While there is no demonstrated direct connection between dental treatment and complications of hypertension it is important for oral health care providers to understand the potential risks and complications that may occur while these individuals are receiving treatment in the dental practice setting. Oral complications associated with taking antihypertensive medications can range from dry mouth, alterations in taste, gingival enlargement, and lichenoid reactions. Evaluation of the medications list and potential side effects may be indicated.
Cholesterol
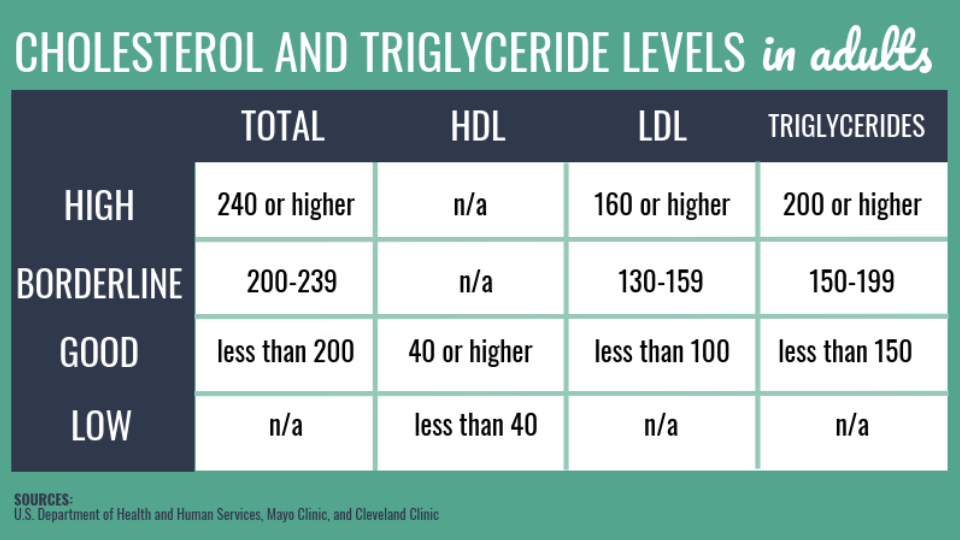
Cholesterol is a waxy substance found in your blood. Your body needs cholesterol to build healthy cells, but high levels of cholesterol can increase your risk of heart disease.
Dental Complications With Cholesterol
Gingival plaque and periodontal attachment loss were associated with elevated levels of systemic LDL/HDL cholesterol and C-reactive protein. In participants treated by statins, this periodontitis-related increase was seen.
Comprehensive Assessment
Clinical Findings:
EO: Within normal limits.
IO: Round, bluish , 1x1mm macule on the left side of the lower lip. Fissured and scalloped, geographic tongue and Palatine torus.
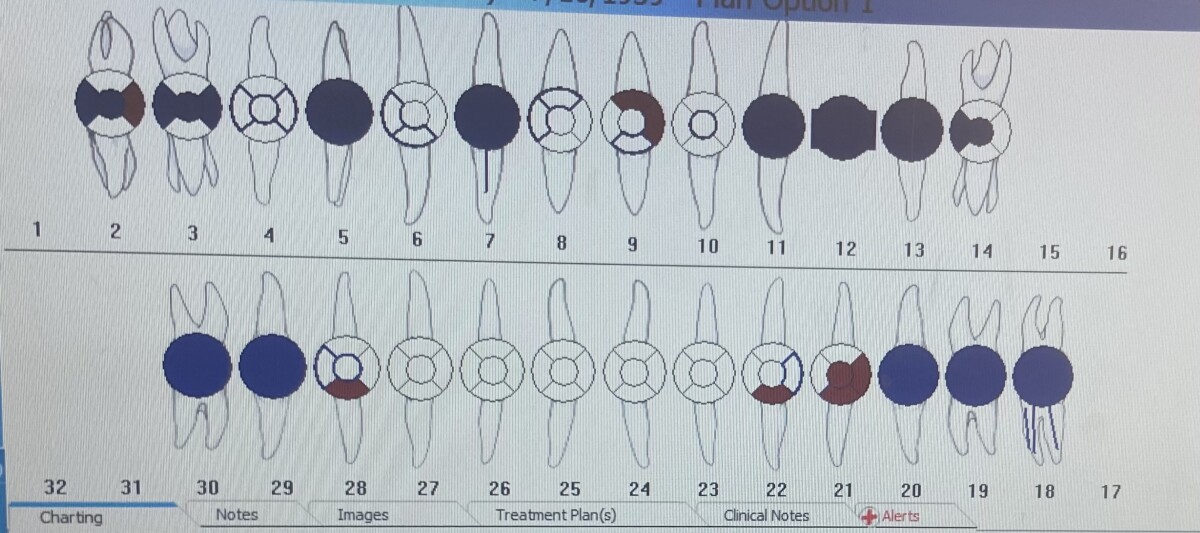
Dentition
- Bilateral Class 1 Occlusion
- Overjet: 4mm / Overbite: 50%
- Fractures/ jagged edges on incised edges of #8 and #9.
- Abfraction on #23F
- Generalized recession.
- Missing teeth #1,#15,#16,#17,#31 and #32.
- Active caries on #2M,#9DF,#21FOD,#22F and #28F
- Patient has composite restorations on all posterior teeth on both arches.
Periodontal
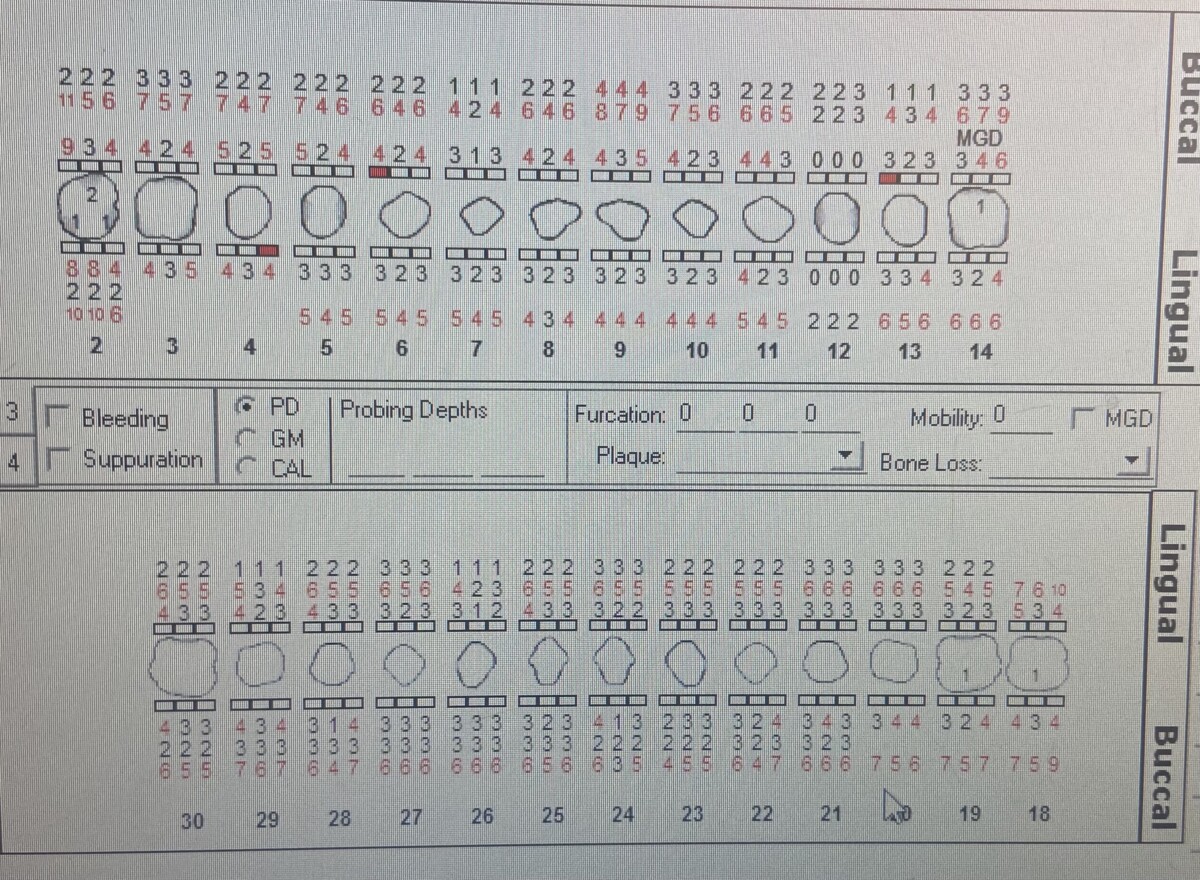
Case type: Stage 2/ Grade B
- Generalized 2-4 mm probing depths with Localized 5-8mm on maxillary and mandibular molar region.
- Generalized 1-3mm recession on all surfaces.
- Localized mild bleeding on posterior premolars and molars.
Gingival Assessment: Gingiva is red/Shiny with moderate generalized inflammation. Rolled gingival margins, blunted interdental papilla, generalized recession with slight bleeding upon probing.
Oral Hygiene
Patient initial plaque score was 1.7 poor with plaque on all surfaces. Medium case value with generalized supra and sub gingival calculus. Calculus was more prominent on mandibular molars.
Planed OHI: On the patients first visit of dental examination the red disclosing agent showed the patient where all the plaque was in his case in all surfaces. Patient stated he has an electrical toothbrush and brushed twice a day. Therefore I introduced to him the proper way to brush with the electrical tooth brush by having the brush bristles at the gingival margin and allowing the brush to do the work and not add pressure which can lead to gingival trama. I also recommend the end-tufted brush to his hygiene care due to plaque on all his distal second molars.
On the patient second visit his plaque index score was 1.6 .The patient stated that he has been implementing the new toothbrushing method and loved the end-tufted brush although his plaque score has not improved as much, what has improved a lot was all the plaque on the distal of the second molars there was little to no plaque which was noted and was told to the patient and was happy to hear since he really like the product. The third aid taught was roper flossing method since most plaque retention was noted in interproximal areas as well.
I emphasized how flossing can help reduce gingival inflammation. I began our conversation by instructing the proper way of flossing: choose right middle finger to hold floss, and excess onto left middle finger of left hand, slide in a short sawing motion, make c-shape against the tooth and use up or down movement.
Radiographs
Radiographs were taken in 2020 but was used to verify active caries lesions and fractures on #8 and #9.


Treatment management
Visit 1
I reviewed patient’s medical history and current medications the patient is taking with follow up questions and intraoral examination were within normal limits. Completion of probing and calculus detection were done. And completed scaling quadrants 1 and 4
Plaque score was 1.7 poor and was taught correct method of using electrical toothbrush also introduced end-tufted brush.
Visit 2
I reviewed his medical history and intraoral examination again- within normal limits. Scaled quadrants 2 and 3, engine polished and applied 5% fluoride varnish treatment.
Plaque score was 1.6. OHI we reviewed the electrical toothbrush method and flossing method.
No medical, social, psychological factors were present that impacted treatment.
I showed the patient the difference in scores and complimented him of his oral hygiene practice. I told him to continue following the instructions provided for tooth brushing and flossing.
Evaluation
The patient was satisfied with his hygiene care although he did not improve much in his plaque index as treatment progressed I showed him where he would need to focus more and this made patient more interested in my instructions.
The patient gingiva at the initial visit was moderate generalized inflammation. Rolled gingival margins, blunted interdental papilla. In the patients last visit the gingival less inflammation and bleeding.
Reflection
I believe I accomplished everything I planned because my patient’s plaque score was reduced. My patient was motivated by the methods I taught and demonstrated. Overall, I was very satisfied because I was able to motivate my patient to conduct health oral hygiene practices.
References
- Xin-Fang Leong, Chun-Yi Ng, Baharin Badiah, and Srijit Das, “Association between Hypertension and Periodontitis: Possible Mechanisms,” The Scientific World Journal, vol. 2014, Article ID 768237, 11 pages, 2014. https://doi.org/10.1155/2014/768237
- Golpasand Hagh, L., Zakavi, F., Hajizadeh, F., & Saleki, M. (2014). The association between hyperlipidemia and periodontal infection. Iranian Red Crescent medical journal, 16(12), e6577. https://doi.org/10.5812/ircmj.6577

