Patient X is an 81 year old caucasian male who presented to the clinic for a routine cleaning. The following breakdown of the case includes gingival descriptions, treatment plan, improvements, intra-oral photos and continued care recommendations.
CC: “Just here for a regular cleaning”
Health History Overview:
-
-
- Vitals: BP reading is within normal limits. 104/62, P: 72.
- Medical conditions: Patient has dementia
- Medications: Gabapentin 100 mg once a day, Finasteride 5 mg once a day, Aspirin 80 mg once a day. Patient previously took valproic acid but reported he no longer takes the medication.
- Social history: Pt doesn’t drink or smoke.
- Dental history: Pt reports using a manual toothbrush 2x/day, uses dentek floss/floss threader, doesn’t use mouth rinse but gargles water after each brush. Pt has no current complaints. PANO was exposed 07/2023. Last dental visit 08/22/2023. Patient brought a form that stated that a resin composite was placed on #9, #21. SDF applied on #12.
-
EO/IO:
EO: WNL, skin dryness.
IO: Posterior bilateral linea alba, white coating on dorsal surface of the tongue. Scalloped tongue. Mandibular bilateral tori.
Dental Charting:
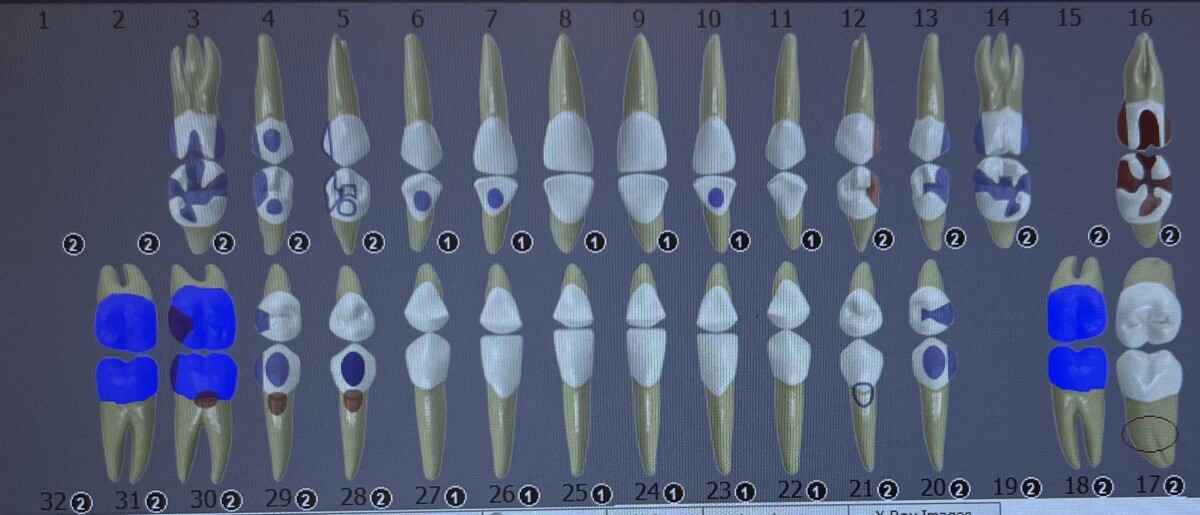
#1, #2, #15, #19, #32 were not clinically present. Metallic onlays were present on #3-MODBL, and #4-DBL. Resin restoration on #5-ODL, #21-B, , amalgam restorations on #6-L, #7-L, #10-L, #13-DO, #14-MODL, #16-O, #20-DOB, #28-B. Porcelain crown on #18, metal crowns on #31, and #32. Buccal restorations on #28 and 29 are gold foils. Suspicious carious lesions on #12, #16, #28, #29, #30.
Occlusion: Class I bilateral classification Overbite: 35% Overjet: 3mm
Gingival description:
Generalized rubbery, pink gingiva with stippling. Hugs tightly around the tooth. Localized rolled papilla on posterior mand/max molars. Generalized blunted GM, embrasures type I. GM appears apical to the CEJ.
Calculus was generalized supragingival, with localized subgingival near the posterior dentition.
Mild yellow/brown staining.
Periodontal charting:

Generalized 2-3 mm PD, with localized 4-5 mm PD on posterior teeth. Localized BOP on mandibular anteriors.
Radiographs:
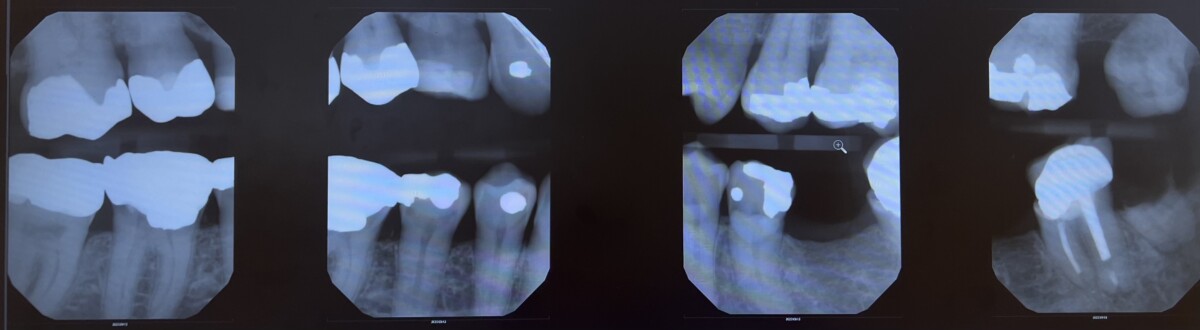
Generalized 20% horizotnal bone loss. Decay on #12-D, retained root #17. Recurrent decay #28-O, #29-MO. Localized calculus #3-D, #30-M. Patient and wife informed of findings.
Dental Hygiene diagnosis:
Periodontal status: Stage II/Grade B
Caries risk: High Case Value: Heavy
Other dx findings: torsoversion
Dental Hygiene Care Plan:
Implementation:
Visit #1: Reviewed medical, social, dental history. Completed dental, period charting. Discussed the use of Listerine Total Care mouth rinse every evening/ Exposed 4 VBWs. provided patient with signed referral for recurrent decay #12-D, #18-torsoversion, #28-O, #29-MO, and extraction of #17 retained roots.
Revisit #2: Completed all assessments. Completely scaled all quadrants with hand instruments and cavitron. Selective polishing on teeth #6-11, #22-27. Another copy of the referral form was given to the patient to follow up with the dentist.
Challenges during treatment:
Modification of the treatment was important for treating this patient. Due to the patient’s dementia status I involved the patient’s wife while explaining any dental findings, OHI, and when requiring signatures for referrals and treatment plan. The patient would forget to swallow resulting in a persistent cough.
To help provide alleviation I sat the patient in a semi-supine position during the treatment and ensured that I was stopping every 2-3 minutes to remind the patient to swallow. We also took several breaks to allow him to sit up and drink water.
I refrained from using ultrasonic instrumentation, however, it was requested by the wife and the patient so I used the ultrasonic for quick lavage and made sure that the patient was seated correctly, and more breaks were used. Due to the patient’s age and hearing quality I also made sure to speak in a slow, loud tone with my mask down so he would be able to hear me and read my lips.
Final reflection:
At the initiation of the appointment I was incredibly nervous about treating the patient. I wasn’t sure what level of dementia the patient had, I wasn’t sure if he would be able to hold a conversation, give consent or even withstand the treatment. However, to my surprise he was an incredibly brilliant gentleman who enjoyed showing me pictures of his paintings and speak about all the memorable events that have happened throughout his life. He was incredibly interested in maintaining good oral health, and his wife was very attentive of him and of his treatment. She was sweet, and gentle with her husband which allowed for a positive, calm atmosphere.
I learned a lot from this patient, and I can definitely say it helped me grow as a clinician.

