Clinic case 1
Caucasian, female, 87 years old. ASA 2
Mrs. B came for a routine check-up and dental prophylaxis. Patient came by herself and walk to the clinic appointment. At the reception area, it was noted the patient had hearing aids and presented an abnormal gait. Vitals were taken. Going through the process of medical history patient stated the COVID-19 vaccine was administered. The last physical examination was 01/20/2021. Mrs. has diabetes type 2 and is taking Metformin 500 mg the last glucose level was 7.3 also is taking Atorvastatin for cholesterol and Aspirin 81mg 4 times a week. Mrs. B was under the care of specialists to control and monitor glaucoma and is taking Brimonidine, Dorzolamide, Timodol, Latanoprost every day. The side effects of the medication are xerostomia and alter taste sensation. Also, is taking multivitamins rebuts the immune system. The patient was neither smoker nor a drinker with no known allergies.
Patient brushes her teeth 2 times a day using Colgate toothpaste, uses toothpicks as interdental aids and rinses 2 times a day with Colgate mouth wash.
Extraoral cancer screening findings unilateral enlarged, soft, and mobile lymph nodes were noted on the right submandibular area, the patient stated that the jaw got locked sometimes. Intraoral cancer screening fissured tongue, bilateral tonsils removed, xerostomia was noted, and redness on the tongue.
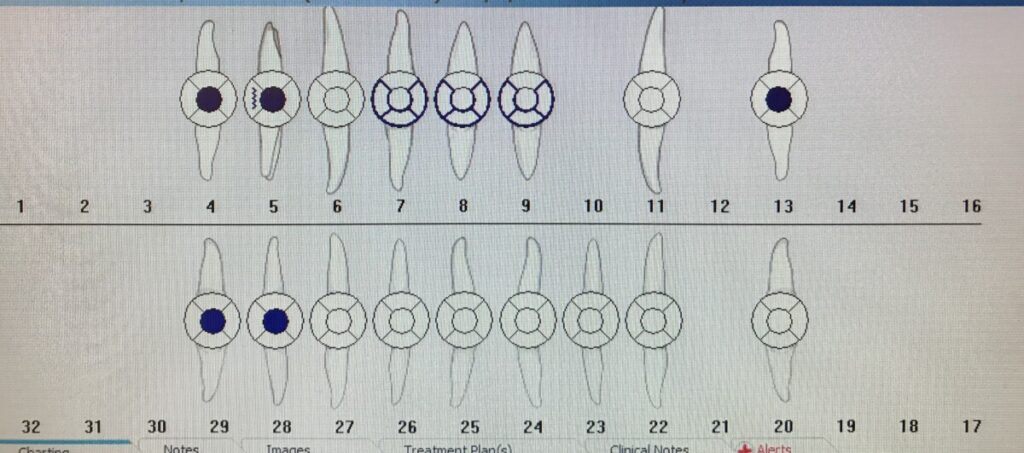
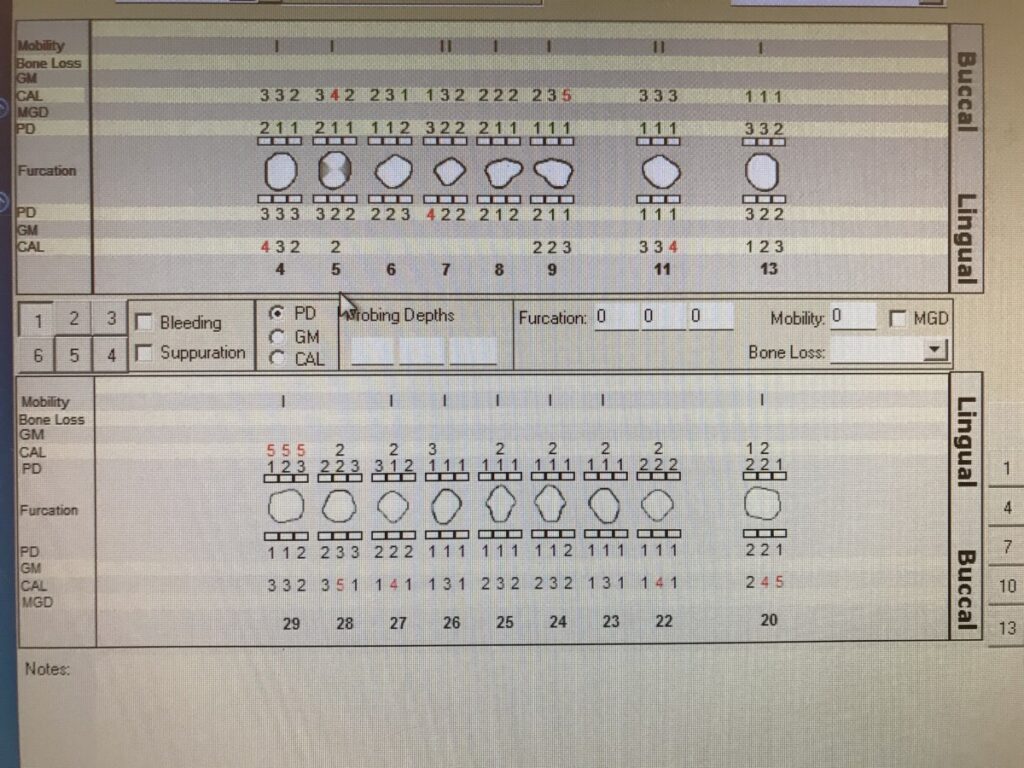
Dental charting several restorations were present such as PMF crowns, implants, and amalgam restoration with open margins, composite, and fractured teeth. The patient complained of tooth sensitivity. Dental charting several restorations were present such as PMF crowns, implants, and amalgam restoration with open margins, composite, and fractured teeth. Patient complained of tooth sensitivity.
Generalized moderated inflammation was present on gingival tissue due to the accumulation of biofilm and improper oral hygiene. PD generalized 1mm – 4mm, localized 5mm and 6mm, localized moderated bleeding, localized recession 2mm, neither tooth mobility nor furcation involvement. Pt complained of sensitivity. Case value was moderate with supra and subgingival calculus deposits and light extrinsic stain. Moderate caries risk due to xerostomia, exposed roots, and multiple restorations. Plaque index (PI) 2 demonstrated poor biofilm removal. OHI, flossing technique was corrected, and a floss holder advised due to limited dexterity. Patient periodontal status was diagnosed as stage 2/B without radiographic evidence.
The treatment plan was presented, discussed with the patient, and kept on 2 visits, and hand scaling only. 20% benzocaine for pain management was the best option. Local anesthetics represent a risk to the patient with glaucoma increases the intraocular pressure.
Mrs. B declined to engine polishing saying, “it will remove the enamel of her teeth” thus, it was removed from the treatment plan. Application of 5% NaFl varnish to prevent caries on exposed roots and tooth sensitivity. During the first visit quadrant 3 was hand scale, and 20% benzocaine was applied for pain management.
The second visit medical history was reviewed, gingival tissue and rescaling evaluation were performed. PI score 2- poor did not present changes from the previous visit. OHI, the Bass toothbrushing technique was recommended and taught to the patient for effective oral hygiene. The remaining quadrants were scaled, 5% NaFl was applied, and post-op instructions were given. Re-care in 3 or 4 months because of improper removal of biofilm.
During the first and second visit, several pauses were made to allow the patient to move and rest in a semi-supine position. The learning experience from these sessions was benzocaine has to be managed carefully on elderly patients, can cause moderate cough when using in excessive amounts. The selection of the questions has to be done carefully since geriatric patients are more prone to provide broad and extended answers. Lastly, to be respectful, sympathetic, and neutral with the ideas expressed by the patient.
Clinic case 2
Hispanic, female, 68 years old. ASA 2
Chief complained, “Want her teeth clean.” Mrs. M was met in the reception area and no abnormalities were noted. Vitals were taken 120/74 under normal limits. Medical history reviewed COVID- status was unknown and vaccines were not available at this time. Ms. M had gastric bypass surgery on 11/2019, with no complications, it was recommended to reduce obesity. Pt has a history of diabetes type 2, cholesterol, hypertension, triglycerides, and pemphigoid. At this time patient was not taking prescribed medication however, the documentation provided by her enlist several medications and vitamins prescribed by her physician. The only medication that was using was Fluocinonide topical for pemphigoid when needed.
The patient was advised to schedule an appointment with the physician.
The patient’s Glucose level was 5.5 under normal levels. The levels of the other conditions have also reduced according to the blood work results 11/30/2020 provided by her. Mrs. M claims that pemphigoid signs and symptoms have diminished.
Pemphigoid an autoimmune mucocutaneous disease, mediated by IgG autoantibodies specific for a desmosomal protein, desmoglein III, resulting in epithelial cell acantholysis. It has no cure. The treatment goal is to diminish the formation and promote healing of the blister in the oral cavity. Anti-inflammatory and immunosuppressor drugs are used to control, but the blisters continue appearing.
Biofilm control and oral hygiene are essential to prevent inflammation of existing blisters and improve healing in affected areas.
Extraoral cancer screening Mrs. M presented excessive skin on the neck area due to loss of weight. Enlarged, mobile, soft, and asymptomatic unilateral lymph node, bilateral crepitation on the TMJ. Intraoral examination, redness on gingival tissue, multiple blisters on the attached and gingival margins cause by pemphigoid, bilaterally enlarged tonsils asymptomatic.
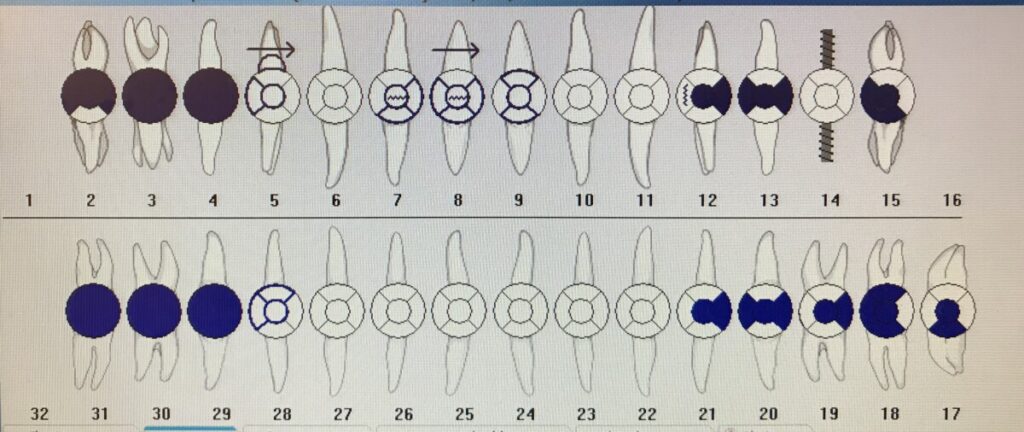
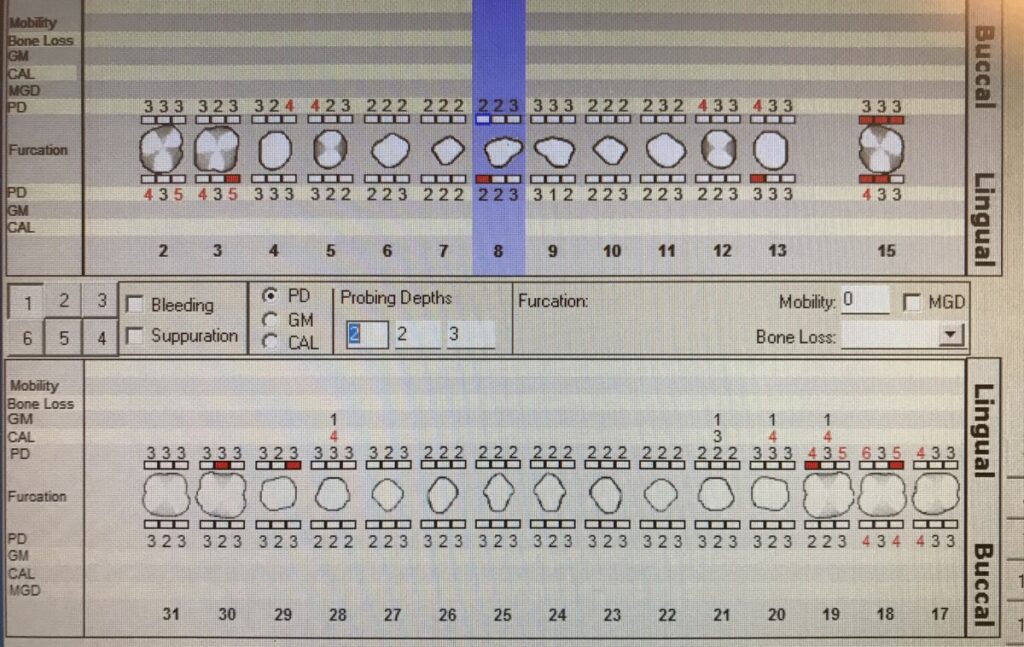
Dental charting missing all molars, multiple amalgam restorations present in premolars. A Dental referral was given to the patient for fracture on #8. PD generalized 1mm-4mm with localized bleeding, generalized 1mm- 3mm recession, 1 and 2mm tooth mobility, not furcation involvement. Case value moderated supra and sub calculus deposits, moderate accumulation material alba. Mrs. M was at high caries risk due to root exposure.
PI score was poor, OHI the Bass toothbrushing technique was taught. The importance of maintaining meticulous dental hygiene care was discussed with the patient. The use of extra-soft bristles toothbrush and oral rinse without alcohol containing to prevent discomfort on the pemphigoid lesions. Also, to keep monitoring the glucose levels because elevated glucose levels can affect pemphigoid increasing inflammation and delaying blister healing. The periodontal classification was determined during this visit.
The treatment plan was discussed with the patient. Prophylaxis was planned to be performed in two visits and hand scaling. 20% benzocaine for pain management, selective engine polishing, and 5% NaFl varnish to prevent caries on exposed roots. In the first visit, not quadrant was scaled. Second visit medical history was reviewed, and intraoral examination was performed. Mrs. M was compliant with brushing her teeth using the Bass technique. PI 1- good and OHI flossing technique was taught and super floss was advised. An FMS was taken base on this the periodontal status was classified as stage 3/c. It demonstrated generalize horizontal bone loss, suspicious caries, and calculus deposits were not noted. Then whole mouth prophylaxis begins, selective engine polish was performed with fine prophy paste, 5% NaFl was applied and post-op instructions were given. Re-care in 3 months.
This patient presented to the opportunity to observe directly the pemphigoid’s effects. Looking at the lesion I could see the difference among another oral lesion such as HSV-1 located in the gingiva. Furthermore this patient required meticulous management of the soft tissue since any lesion could exacerbated the effect of pemphigoid, cause new blisters.