
CASE #1
The patient is Z.Y.X, 22 years old female, Ortho patient (since 10/2015). M/I. No significant findings in patient’s medical history. Patient is a non-smoker, has no systemic conditions, and patient is not taking any prescription medicine or any over-the-counter (OTC) medication. BP was 101/70, pulse was 76. ASA I.
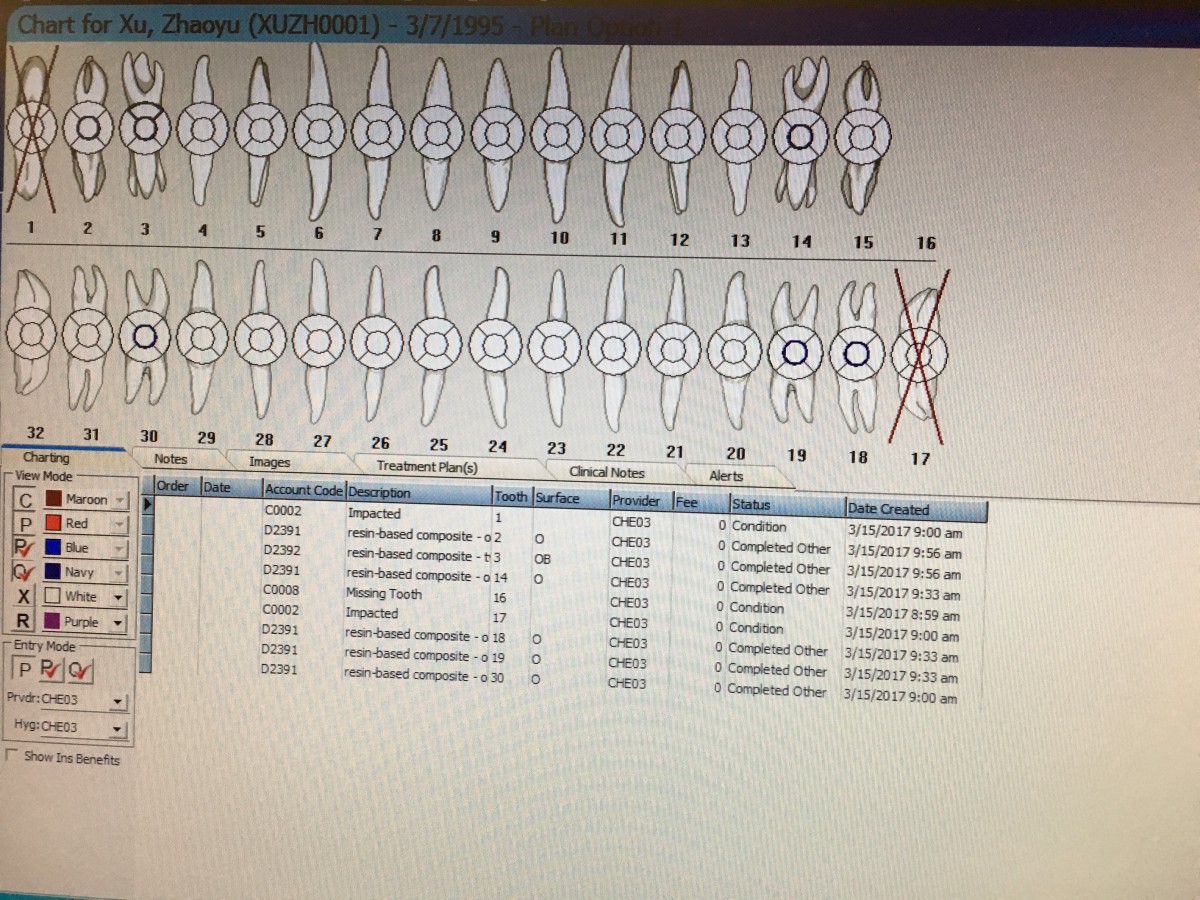
There were no clinical findings of attrition, erosion, abfraction, or abrasion. Composite restorations on tooth #2-O, 3-OB, 14-O, 18-O, 19-O and 30-O. Imapcted tooth #1 and 17. Missing tooth #16. There were no active caries. Generalized healthy gingival tissue. The gingiva was pink, firm, resilient and pointed interdental papillae. The patient’s probing depths were generally 2-3mm. There was minimal bleeding upon probing (BOP) and slight inflammation at the posterior region. There was no clinical attachment loss and no recession present on this patient.
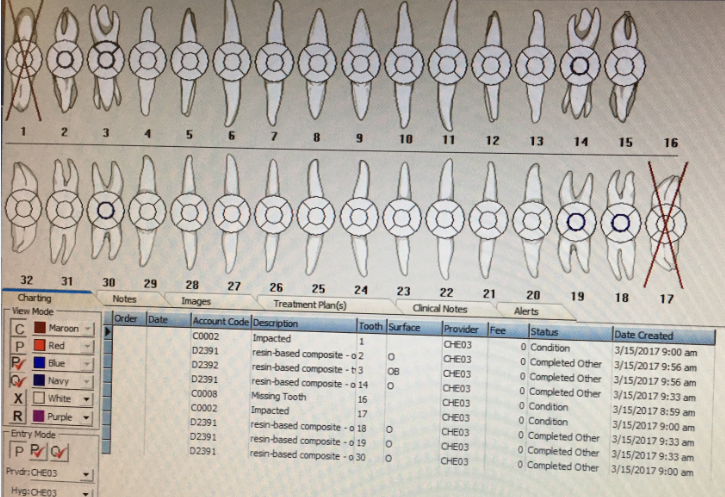
Dental Charting
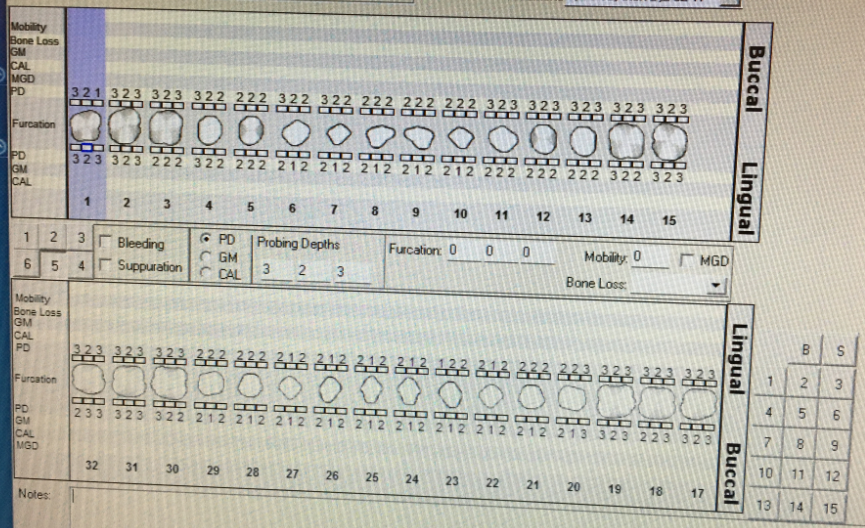
Perio Charting
The patient was classified as a medium based on calculus present. Localized sub-gingival calculus deposits on mandibular lingual and maxillary posterior region. Accumulated biofilm.
Panoramic radiographs was exposed on 06/2016 in dental office.
OHI, superfloss was recommended due to plaque accumulated on the interproximal area and around the braces. I scaled the full mouth by using ultrasonic and hand instruments. Air polishing was adapted on the patient. Also, fluoride treatment, 2% NaF for 4 min. Recall visit in 6 months due to her medium case type.

Before (accumulated biofilm)

After (air polishing)
CASE #2
The patient is M.T.L. 19 years old female. H/I. No significant findings in patient’s medical history. Patient is a non-smoker, has no systemic conditions, and patient is not taking any prescription medicine or any over-the-counter (OTC) medication. BP was 101/68, pulse was 80. ASA I.
2×2 mm lesion was present near tooth #16 buccal mucosa which present as small and red. Patient reported no painful.
There were no clinical findings of attrition, erosion, abfraction, or abrasion. Patient is missing teeth # 1 and 32. Amalgam on tooth #3-O and composite restoration on tooth #19-O. There were no active or suspicious caries. Generalized healthy gingival tissue (pink, firm, resilient and pointed interdental papillae). The patient’s probing depths were generally 2-3mm and have localized 4mm pocket depths on posterior molars region. Periodontal type I. There was minimal BOP and slight inflammation at the posterior region. There was no clinical attachment loss and no recession present on this patient.
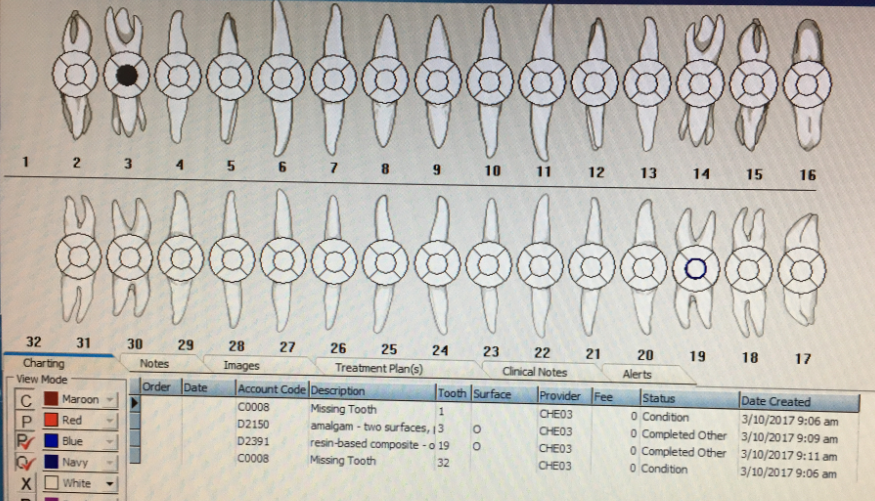
Dental Charting
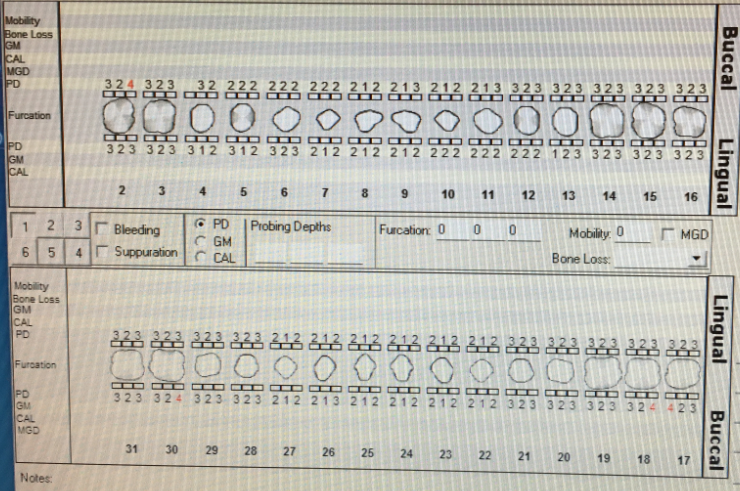
Perio Charting
The patient was classified as a heavy based on calculus present. Localized sub-gingival calculus deposits on posterior region and anterior lingual. Localized supra-gingival calculus on posterior teeth. Heavy stain present.
The patient’s last dental x-rays BWs was exposed 6-8 months ago. Patient’s 3rd molars, tooth #1 and #32 were not seen clinically, tooth #16 and 17 were impacted. So Digital Panoramic radiograph was recommended to the patient for further examination. Panoramic radiograph was exposed on March 10, 2017 in clinic. It reveals impacted and malposed third molars. A referral form was given to the patient for oral surgery examination.

Digital Panoramic Radiograph Exposed on 03/10/2017
OHI, the most plaque was accumulated near the cervical third and around the gingival margin. Therefore, Modified Bass Method was recommended and instructed to the patient.
I scaled the full mouth by using ultrasonic and hand instruments. Based on my analysis and interpretation of the data gathered during the assessment, the patient has heavy stain presented.

Stain presented on Maxillary lingual
Therefore, engine polishing (coarse paste) was applied on the patient to remove the stain. Also, Fluoride treatment, 2% NaF for 4 min applied after polishing. Recall visit in three months due to her heavy case type.


{kind=link}