The patient is a 31-year-old African American male and is ASA II due to daily smoking of marijuana, per patient. The patient also stated that he has ADHD, and does not take medications. The patient uses a soft manual toothbrush “usually twice a day” with peppermint toothpaste, flosses with floss picks and uses Breath-Away mouth rinse daily. The patient had a dental visit in July 2022 and had a panoramic x-ray exposed at that time. His last dental cleaning was in July 2009. The patient also mentioned having dry mouth, likely due to “cotton mouth after smoking.”
The extra-oral examination showed no significant findings, all were WNL. The intra-oral examination showed bilateral linea alba and erythematous tonsils. The patient also had a localized moderately erythematous line along the gingival margin of the mandibular posterior lingual teeth, inflamed gingiva on his mandibular anterior lingual teeth, and moderate bleeding. He was determined as a Heavy case with gingivitis.
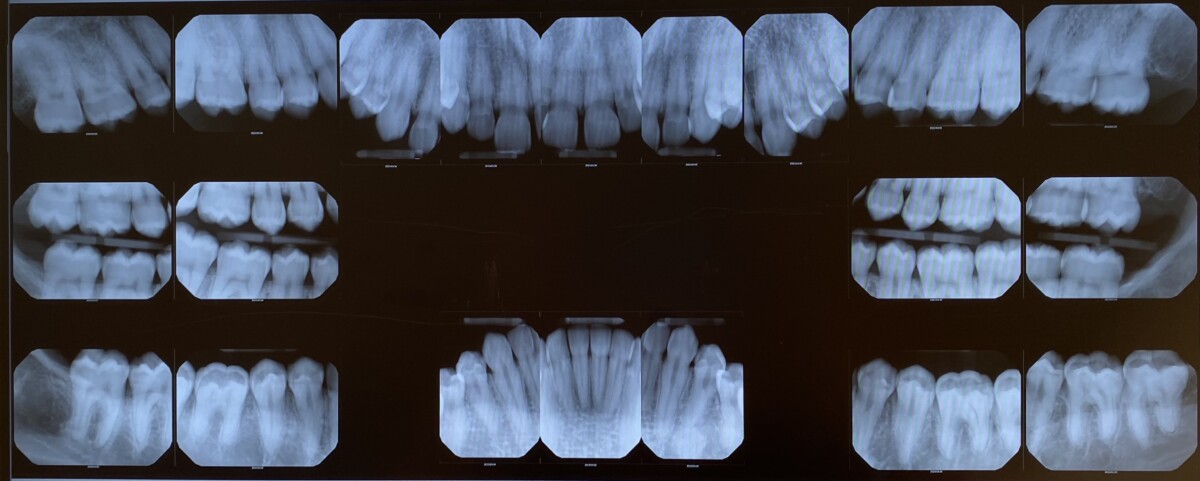
His PI score at the initial visit was 1.67 (fair) and remained the same at the revisit, unfortunately. The Modified Bass brushing method was demonstrated, as the disclosing solution primarily remained on the facial/buccal surfaces of the teeth rather than the interproximal. The brushing method was reviewed on the revisit, and the proper flossing method was demonstrated as well. While giving oral hygiene instructions, I also explained that the effects of smoking, such as dry mouth, can cause caries to form and lightly suggested that he could change his habits or drink more water so as to combat the dry mouth effect. A full-mouth series was also exposed, noting a few interproximal caries as well as periapical pathology (PAP) on #21, both of which a referral was given. The treatment was completed, 5% Sodium Fluoride varnish was applied and post-op instructions were given. Ultimately, the patient seemed to understand how smoking can affect his oral health; however, I am unsure as to whether he will change his habits.