
Demographics:
Patient is D.T 31 years old, Heavy/ Type II.
Assessment:
Patient was hospitalized February 2016 due to kidney stones. Patient reported he was treated for kidney stones and he no longer has this condition. Patient was required to take oxycodone for a week and a half to treat pain caused by the kidney stones. Patient states he suffers from phobias and from chest pains due to alot of severe stress. Patient stated having no specific phobia. Blood pressure was 142/86 and pulse was 93. Referral was given to patient for blood pressure. Patient is an occasional smoker. No premeditations were needed. No medications were being taken at that time of the appointment. No systemic conditions. ASA II.
Oral Pathology:
Extra oral examination revealed TMJ was present. Cracking upon opening/ side to side movement of his jaw. Patient stated he feels comfortable and has no pain.
Intra oral examination revealed that the patient had patechia adjacent tooth #16, Linea Alba present adjacent to tooth #16, and Lingual root tip adjacent to tooth #4. Tonsils were also inflammed, patient stated he was aware.
Dentition
Patient’s Class of occlusion is I, overjet 0mm, and overbite 0%. Patient only missing tooth #1, no restorations were found. Active carries were found on tooth #3 distal occlusal surface and tooth #17 distal occlusal surface. Patient present with attrition on tooth #6,11,22,27,8,9,25,24.
Periodontal
Patient is a type II localized type III. He had generalized 3-4mm probing depths, localized 5-6mm in posterior areas. No recession present. Severe bleeding upon probing and severe inflammation was detected.
Gingival description appeared coral pink, bulbous, resilient, smooth, severe inflammation generalized.
Oral Hygiene
Patient had generalized supragingival calculus on maxillary and mandibular teeth lingual and facial surfaces. Subgingival calculus was detected generalized on both maxillary and mandibular facial and lingual surfaces.
After explaining what a plaque score is, and showing examples of plaque score on my flip board. I explained what plaque and calculus was to my patient. I interviewed the patient on the patient self-care. The patient’s initial plaque score came out to be a 2.3. Plaque was shown interproximal, facial and lingual. I showed the patient modified bass as first choice because he had so much plaque on facial surfaces and told me he does not brush daily. On the second visit the patient plaque the score went down to a 2, I then demonstrated flossing technique due to marginal, interproximal plaque. On the last visit the patients plaque score was a 0.6. I reevaluated flossing and modified bass with the patient and asked him if he had any difficulty or problems with either method, his response was no.
Radiographs
The patient hasn’t been exposed to x-rays since 2006. The patient was recommended to have a full mouth series taken. Full mouth series was not exposed but the patient agreed to come back to have x-rays taken.
Treatment Management
During the first visit assessments. The second visit, modified bass was demonstrated. I hand scaled and used my cavitron on the LRQ. LRQ was completed by the end of class and checked by faculty. On the third visit the LRQ and brushing was evaluated and flossing was introduced. URQ and ULQ was hand scaled and cavitron was used to completion and checked by faculty. On the fourth visit brushing, flossing was reevaluated along with LRQ, URQ, and ULQ. LLQ was hand scaled to completion. Polish was done on the fourth visit as well. Patient refused fluoride. Patient was recommended for a three-month recall.
There were no medical, social, or psychological factors impacting treatment.
Patient stated that he tried to floss and brush at home more than he is use to. His plaque score each time decreased so it showed he was brushing and flossing daily. Patient was referred for blood pressure. I would not have changed any part of my treatment or patient education because i felt i worked well chair side with my patient, he stated he was content with each appointment we had.
Evaluation
When first meeting this patient and going through assessments I felt so overwhelmed. I did not know how I was going to handle him. Just speaking to him I saw how severe his gingiva was inflamed and how much calculus he had on his facial surfaces of his teeth. Speaking to him he was not into his oral health at all. After a few visits of encouraging him and showing him what his gingiva and teeth can look like he seemed much more into his oral health. On his first visit when I taught modified boss he did not even know how to hold the tooth brush and showed massive pressure applying the tooth brush to his teeth. With my help and encouragement I explained to him that the angel of the toothbrush would help get into his gum line and reach the plaque below the gum line as well as above it. He seemed to really like that brushing technique. When he came back on his second visit his plaque score went down and he told me he had found brushing beneficial. When I taught him flossing he found it difficult but we went over it until he understood the “C” shape, up and down method. By the last visit the patient’s gingiva was less bulbous firm and more pink. I was so surprised how much better it looked in the matter of a few weeks. After giving my patient his take home care package he seemed determined to keep up with his flossing and brushing method daily. When I told him to come back in 3 months he sounded firm about coming back to get a cleaning and x-rays done.
Reflection
I was able to accomplish everything I planned with my patient both educationally and clinically. My patient took my recommendations home and applied them himself. I learned a lot from this patient being that he was a difficult, and not into his oral health at all. He was such a heavy patient but the best experience I had all semester. I was very patient and encouraging toward him. Together we improved his oral health, which was very satisfying. He also complimented me in front of one of the Professors I had that day and stated he would love to follow me into my future practice because he felt so comfortable and well taken care of. After completing this patient I felt more confident and happy about how I got to help him improved his daily oral health. My strengths with this patient was being so patient and learning to deal with a difficult patient. My weakness was time management but I handled the appointments as best to my ability and the best to his comfort. Overall this patient was a great experience and I enjoyed helping him on his journey to a happy and healthy smile.

( This picture shows that the LR quadrant has been scaled in comparison with the others.)
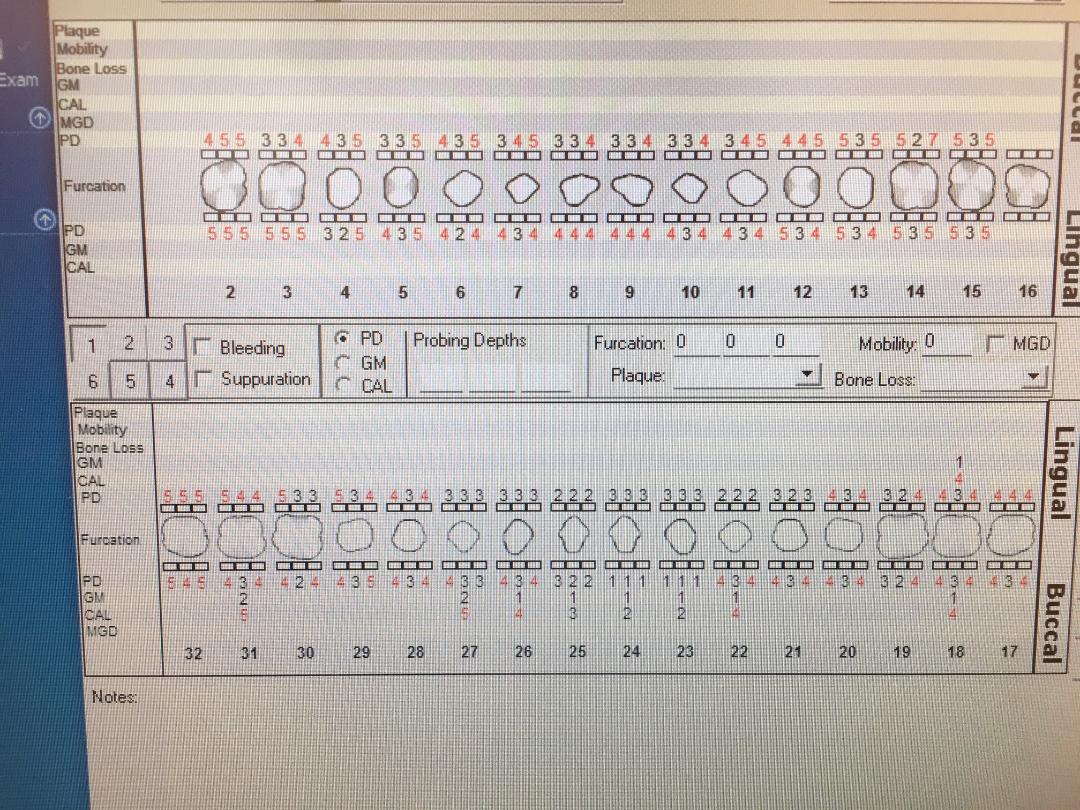
(Patients probing depths- Generalized Heavy/type II.)
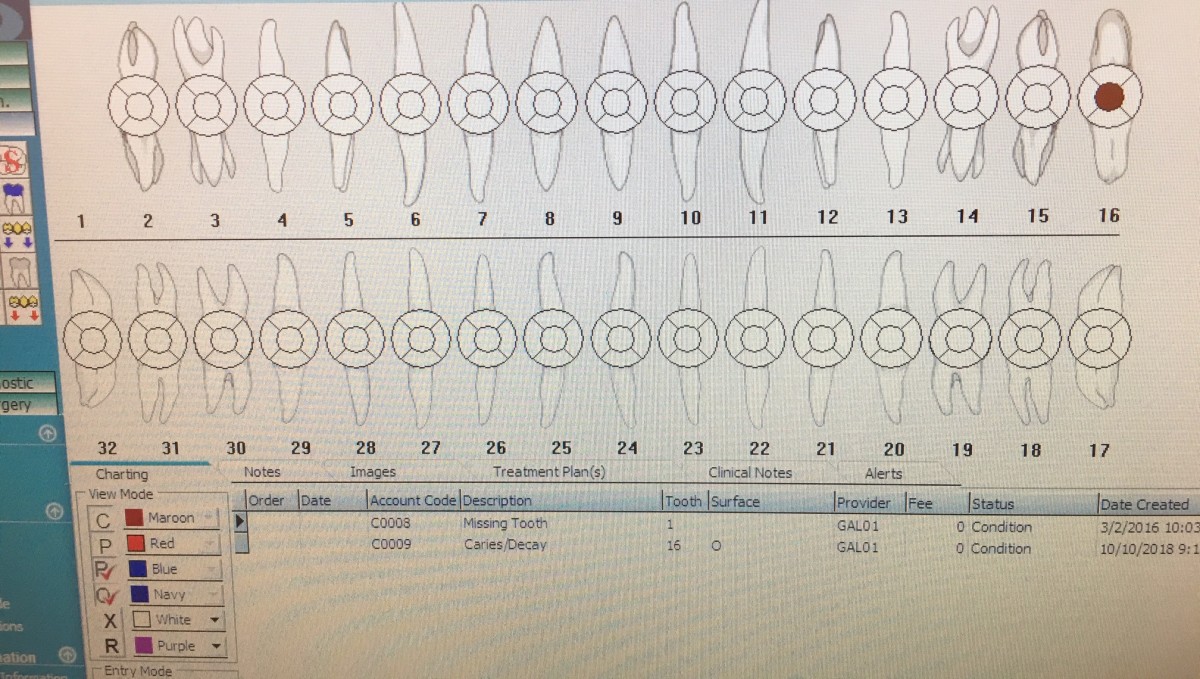
(Patient’s dental charting.)

