Case Studies
Case Study I – Arestin Treatment
Recare/L/II- A 55 year old caucasian female, healthy, non smoker, no systemic conditions, no medications. ASA I
Dentition: Orally presented with generalized amalgam restorations, four porcelain fused to metal crowns.
Periodontal: Patient’s gingiva was pale pink, spongy, and pyramidal. Patient is classified as Type II Periodontitis with radiographic evidence of bone loss and localized recession, she presented with 3-6mm PD with minimal inflammation and moderate BUP. Patient has light calculus deposit present on the lower anteriors and interproximally in the posterior. Patient qualified for Arestin treatment due to her BUP and pocket depths ranging from 5-6mm in the mandibular posterior areas.
The treatment plan consisted of 3 Visits:
- Visit 1: Completion of all assessments. OHI- Flossing 1xday, brushing 2xday recommended an electric toothbrush and rinsing with Listerine Antiseptic-10ml for 30 secs daily. Patient was exposed to FMS in 2016 to evaluate the bone loss as Type II perio, and no caries were found. Patient qualified for Arestin (which was placed on the second visit) Scaled all 4 quadrants using ultrasonic and hand scalers, engine polished, and applied 5% Fluoride Varnish treatment.
- Visit 2: Re-evaluation of all 4 quadrants that were previously scaled checking for any residual calculus present and tissue response. Patient responded positive to treatment interventions from last visit. Patient stated that she was incorporating flossing and purchased an Oral B electric toothbrush that I had recommended. Patient’s tissue responded well it was resilient with less bleeding upon exploring and minimal inflammation, as well as pocket reduction in her localized 4mm PD’s. Arestin was placed on six sites #18 DB[5mm], MB[5mm], B[5mm], ML[5mm], DL[5mm] and #30 DL [6mm]. Verbal post instructions as well as written post instructions for Arestin placement was sent home with the patient.
- Visit 3: Re-evaluation of the areas where Arestin was placed. Patient’s tissues and PD have responded positive in the areas where Arestin was administered. The patient’s gingiva was pale pink, firm, resilient, and pyramidal. Patient had no BUP and patient presented with a pocket reduction with 1-2mm difference from previous visit. Patient was put on a 4 month recare.
After post Arestin re-evaluation was completed, we discussed the remarkable results from the Arestin treatment and how important her compliance of home care has played a major role in the success of the Arestin treatment. The patient was very pleased with her results, and I encouraged the patient to keep up with her daily oral hygiene home care. I was very static that the patient became very compliant and completely changed her old habits for the better, as well as taking her oral health seriously.
Case Study II
New Patient/H/I- A 25 year old african american female who has Anemia and low vitamin D deficiency. Patient states that she has a heart murmur. Patient had an echocardiogram test for it, and states that she isn’t sure what type of murmur she has but was told that her doctor will keep an eye on it. Patient also has seasonal allergies to pollen and mold. ASA II. After performing a thorough extra-oral and intra-oral examination, she has a slight crepitation on the left side of her TMJ, presents with exostosis on the maxilla, a high vaulted palate, and pronounced mandibular tori on the left side.
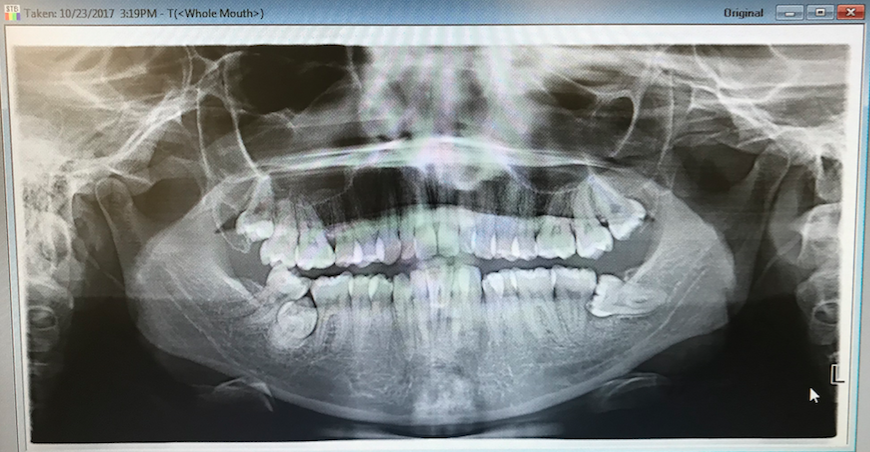
Dentition:Patient had attrition on #4-5,12-15,20-23. Tooth #16 was partially erupted. After patient was exposed to a PAN it was radiographic evidence that #1 and #17 were impacted as well as tooth #31 was partially impacted in between #32, and #30.
- Referral was given to see an oral surgeon for #1,17,and #31 for an evaluation
Periodontal: Gingiva is pigmented and red with generalized marginal inflammation, bulbous and flaccid on #30-32. Patient is classified as type I gingivitis with radiographic evidence of no bone loss. She presents with 2-4mm PD with localized 5mm PD in the posterior. Patient had moderate BUP and moderate inflammation.
Patient was a heavy case value; She presented with generalized surpragingival and subgingival calculus on both the maxilla and the mandible.
Her plaque score was fair. Patient stated that she never flosses and brushes aggressively using a manual tooth. I recommended using an electric toothbrush and start flossing 1x a day as well as use and antiseptic rinse as an adjunct to brushing and flossing.
Radiographs: Patient was exposed to a PAN and 4 BWS due to the patient not having a baseline of radiographs since 2013. A PAN was required to see if #1, #17 and #31 were impacted as well as 4 BWS to see if there was any interproximal caries present.
- The BWS confirmed there was no radiographic bone loss or caries presented.
- The PAN confirmed that #1 and #17 where impacted and #31 was partially impacted. This can be the reason why the gingiva is flaccid in that area due to the tooth trying to erupt and as well as food getting impacted in the area.
The treatment plan consisted of 3 visits:
- Visit 1: Completion of all assessments, OHI, plaque score, and recommended the patient to use an electric toothbrush. The patient presented to me that she brushes aggressively with a manual toothbrush. I explained to her when you use an electric toothbrush it automatically corrects you to use light pressure and the toothbrush does all the work for her. During this visit I spent time with her to educate her on the importance of oral hygiene since she stated to me that every time she has gone to the dentist no one ever took the time to review oral hygiene.
- Visit 2: OHI, plaque score. Patient stated that she bought the Oral B electric toothbrush and she loved it. I also introduced flossing using the REACH shred resistant and conventional floss explaining to her the importance of removing the biofilm every night so it does not calcify overtime. I exposed the PAN and reviewed the radiographs with her and referred her to see an oral surgeon to evaluate #1,17 and #31. I then proceeded and hand scaled and ultrasonic the UR and LR with 20% benzocaine topical.
- Visit 3: OHI, plaque score was good, Patient was being complaint at home, and her gingiva had dramatically changed since her first visit. I recommended using Listerine Antiseptic as an adjunct to brushing and flossing to kill the bacteria that causes gingivitis. Reevaluated previously scaled areas. Exposed 4BWS, and completed all 4 quadrants using ultrasonic and hand instruments, engine polished with fine paste and applied 5% sodium varnish. I placed her on a 6 month recare.
Patient responded very passionate to treatment interventions, she explained to me that she felt such a difference in her gingiva as well as seeing a difference in the appearance of her teeth. I had an overall effective experience with this patient who was very willing to make a change and learn new interventions when it came to learning about the importance of optimal oral health.

