The following are clinical journals/reflections written on 3 separate cases I managed during my clinical experience at City Tech:
Case 1
EG, 60, M/III
- Patient Health History
This patient has a health history of anxiety and depression, and is taking prescribed medication to manage conditions. The medications are Effexor XR, 225mg q.d, and Trazadone, 150mg q.d. Both drugs are selective serotonin and norepinephrine reuptake inhibitors (SSNRIs). Dental effects of medications include: increased bleeding, nausea, postural hypotension, and xerostomia. This patient stated she had a previous adverse reaction to the epinephrine in Lidocaine, so the local anesthetic indicated is Carbocaine. No other allergies or systemic conditions were marked or observed, and the patient presented with a BP of 100/64 with pulse of 72 bpm. This patient had an ASA II classification because of her age and medical condition with Rx. - Oral Pathology
None present. - Dental
This patient had light incisal attrition on #7-11, and #23-26, with light abrasion on #11 facial. This patient had an anterior crossbite with Class I occlusion on the left and class III on the right, a 3mm overjet on the right and 2mm on the left, and a 10% overbite. This patient is missing #1, 4, 5, 12, 14, 16, 17, 19-21, 28, 31, and 30, and #29 has been restored with an implant. The lingual wall of #18 was fractured completely. No caries detected clinically. - Periodontal
Patient’s gingiva was light pink, with bulbous margins, blunted papillae, and was spongy and retractable with an amalgam tattoo in the edentulous area between #3 and #6. This patient has active refractory periodontal disease with 2-6mm pockets, exposed furcations on #18 and #30 buccal, and class I mobility in #18, with light generalized bleeding on probing. This patient has generalized recession of up to 5mm on buccal aspects of canines and molars, with mucogingival defects on #18 and #30. Her periodontal classification was determined a generalized Type III. Arestin is not an appropriate treatment for this patient as her CAL is too great with recession, and she is not compliant with homecare. - Oral Health
This patient was classified as a Medium based on calculus deposits present. Calculus deposits were tenacious and located subgingivally around maxillary and mandibular molars, and supragingivally around maxillary and mandibular anteriors, with moderate staining. Patient had food debris lodged interproximally and in vestibules. Her plaque score was a 1.2 with most of her build-up on the lingual and interproximal tooth surfaces. Upon interview, patient stated she uses a manual toothbrush only once per day, and does not use an oral rinse to control oral microbial load. - Radiographs
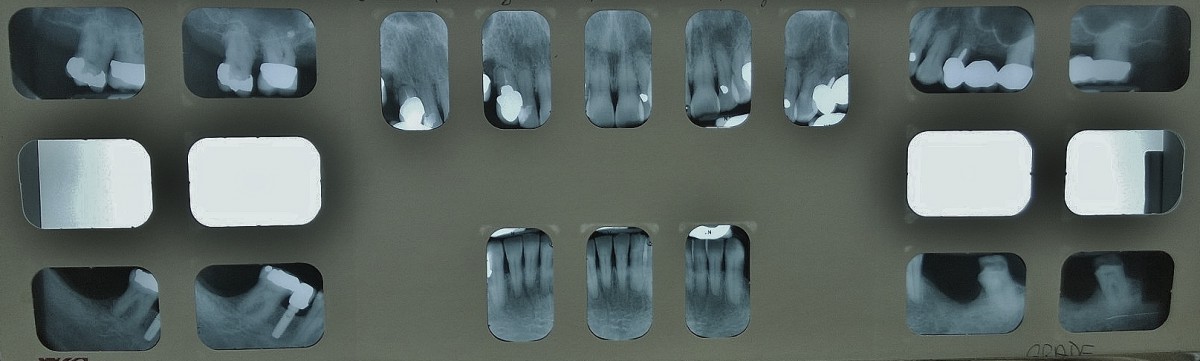
This patient required a full mouth series of radiographs with vertically oriented bitewings, which I exposed on her revisit appointment. The radiographs supported the clinical findings, and did not reveal anything additional aside from a better visual of her level of bone attachment.
Other Findings
This patient does not smoke or drink alcohol at all, but has a past history of alcoholism and is 20 years sober. This patient is economically unsound, lacking dental insurance or a means to afford therapeutic treatment. She is also psychologically unsound, often cycling through period of depression. All these factors may affect this patient’s outcome in reaching optimal health.
TIME: The time interval between the patient’s last recall visit and this one was 5 months. A more appropriate time span would have been 3 months, however the 3 month mark would have been July, and our clinic was not open until September.
TREATMENT MANAGEMENT: On the first visit, I reviewed oral hygiene instruction with the patient, and scaled her upper right and lower right quadrants using 2 carpules of Carbocaine for pain management. On the second (and final) visit, I exposed a full mouth series of radiographs, reviewed oral hygiene instruction and scaled her upper left and lower left quadrants using 2 carpules of Carbocaine, polished, and applied fluoride varnish. I stressed to the patient the importance of mechanical disruption of the biofilm AT LEAST twice daily, and that she should consider switching to a power assisted toothbrush for more effective debris removal. I also advised she also begin using an alcohol free antimicrobial rinse, such as Crest Pro Health. However, with the new information learned since during the semester, I would probably recommend a chlorhexidine rinse twice daily for 1 week, followed by a fluoride rinse and/or Biotene to manage the side effects of her medications and promote gingival health through bacterial disruption. Patient seemed interested in information and promised to begin implementing recommended homecare interventions immediately, however she promised the same last semester and her gingiva did not improve much between her April and September visits. I’ll find out in December at her month recall if I was able to get through to her this time. This patient was referred to a dentist for evaluation of #18 and fractured lingual wall, and to a periodontist for evaluation of perio. disease.
REVISIT EVALUATION: At the patient’s revisit appointment, her plaque score decreased to a 0.6. She claimed to be brushing and flossing more frequently, but had not yet purchased the Crest Pro Health rinse. Her tissue was still blanched and spongy with retractable margins, and there was light bleeding on exploring. The patient seemed less interested in her oral hygiene during this visit and more interested in finishing up quickly. She was antsy and kept asking how much longer and if I would complete her that day. At this appointment I exposed a full mouth series of radiographs, reviewed oral hygiene instruction, scaled her upper and lower left quadrants using 2 carpules of Carbocaine, polished with a fluoride paste, and applied 5% NaFl varnish to manage dentin hypersensitivity on exposed root surfaces.
Case 2
AN, 24, H/I (II)
- Patient Health History
This patient has no known allergies or systemic conditions, and no history of past illness or injury. He presented with a BP of 100/64 and pulse of 72 bpm. This patient had an ASA I classification because he is under age 60 with no history of illness, injury, or medication/drug consumption, and he presented with vitals within normal limits. - Oral Pathology
None present. - Dental
This patient has incisal attrition on #6-12, and 22-27, and light facial abrasion on #21, 28, and 29. He had bilateral partially-erupted mandibular 3rd molars, and active caries were suspected on #2 O, 11 and 12 F, and 30 B. This patient is at high caries risk level because he presented with over 3 carious lesions, drinks soda frequently, has exposed root surfaces, and has more than one interproximal restoration. - Periodontal
Patient’s gingiva was red, bulbous, spongy, and retractable. His probing depths were 1-4mm with light bleeding on probing. He also presented with 2mm recession on #18-21, and 28-31 F. He was classified as generalized Type I gingivitis, however I think he should be a Type II slight periodontitis because of his multiple 4mm pockets, mandibular facial recession, light bleeding on probing, and slight radiographic bone loss. Arestin would be appropriate for this patient because he had moderate inflammation with 4mm pockets. - Oral Health
This patient was classified as a Heavy based on the quantity of calculus deposits and staining present. Calculus deposits were located both sub- and supragingivally around mandibular anteriors, and supragingivally throughout the dentition, with moderate staining. His plaque score was good, 0.6 with the most accumulation on the mandibular lingual surfaces. Upon interview, patient stated he uses a manual toothbrush twice per day, flosses occasionally, uses nothing to clean his tongue, and rinses with a 0.2% chlorhexidine digluconate mouthrinse. - Radiographs
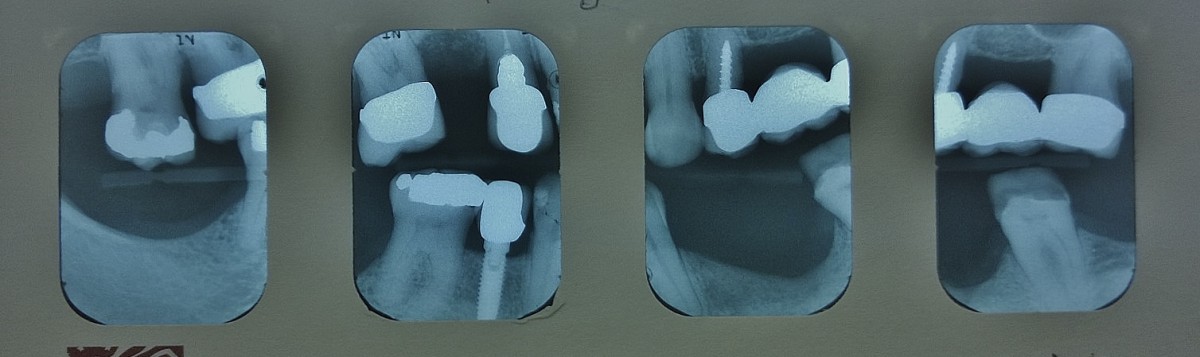
This patient required a full mouth series of radiographs which I exposed on his revisit appointment. The radiographs supported the clinical findings, and did not reveal anything additional aside from a better visual of his level of bone attachment, and rule out radiographically-visible interproximal caries.
Other Findings
This patient lives in England, and was only in this country visiting. This, to his knowledge, was his first dental prophylaxis/preventative dental treatment. I had to look up his mouthrinse, brand name: Corsodyl, to learn it was a chlorhexidine rinse. He said he purchased it over the counter and it was not prescribed. He drinks diet soda and tea heavily. All these factors may affect this patient’s outcome in reaching optimal health.
TIME: This was the patient’s first dental hygiene appointment. This is not an appropriate time-span, and his first hygiene visit should have been well before age 24.
TREATMENT MANAGEMENT: On the first visit, I gave oral hygiene instructions to the patient, and scaled his upper right and lower right quadrants. On the second (and final) visit, I exposed a full mouth series of radiographs, reviewed oral hygiene instruction and scaled his upper left and lower left quadrants, polished, flossed, and applied 2.5% NaFl foam. Upon his return home, I recommended the patient discard his toothbrush and use the one I provided to him and continue with soft-bristled brushes from thereon. I taught him the modified bass technique and stressed that he avoid lateral brushing especially on the mandibular facials, and to use a gentler amount of pressure while brushing. I also recommended he look at what electronic toothbrushes are available in England, and consider switching to an e-brush for more efficient toothbrushing. I encouraged the patient to floss daily, to brush or scrape his tongue, and to look for a fluoride-based mouthrinse to use at home instead of the Corsodyl. I made the patient aware of his carious lesions and how his frequent diet soda, and sugared tea ingestion impact the frequency and progression of those lesions, and ma sure he understood he needed to both implement a source of fluoride into his daily routine and decrease the frequency he drinks acidic and sugary beverages. The patient was given a referral, along with a copy of his xrays, for caries evaluation of #2, 11, 12, and 30.
REVISIT EVALUATION: At the patient’s revisit appointment, his plaque score decreased to a 0.3. This appointment was only 2 days after his initial appointment, but he said he had implemented the new brushing technique, and flossed since his last visit. His gingival tissue was still red, with pale margins, bulbous, and spongy with no bleeding on exploring. The patient showed interest in his state of improvement from first and second visits, and appeared motivated to continue with his learned techniques. He asked questions and was thoroughly impressed by the before and after visual of his mandibular anterior lingual surfaces in the mirror. At this appointment I exposed a full mouth series of radiographs, reviewed oral hygiene instruction, scaled his upper and lower left quadrants, polished with a fluoride prophy paste, flossed, and applied 2.5% NaFl foam.
Case 3
JG, 43, H/II
- Patient Health History
This patient was diagnosed with hypertension 1 year ago. He takes 5mg/day prescription Enalapril, an ACE Inhibitor, for management of hypertension. This drug can cause abnormal taste and orthostatic hypotension, which are dental treatment concerns; it also has side effects of dizziness and renal disease. Enalapril should not be combined with other antihypertensives, Lithium, or antacids. He also has an allergy to Penicillin. The patient’s blood pressure was within normal range at: 115/69, pulse 58. - Oral Pathology
None present. - Dental
This patient has attrition on #6-11, 22-27, and light facial abrasion on #21, 28, and 29. He had no restorations, but was missing #1, 9-13, 18, and 20; and used a removable dental prosthesis to fill #9-13. He was not caries active. - Periodontal
Patient’s gingiva was red, bulbous, spongy, and retractable. His probing depths were 2-6mm with 4-6mm around the maxillary and mandibular molars, with moderate bleeding on probing. He had 2mm recession on #21, and 28 F. He was classified as generalized Type II early periodontitis, because he had 4-6mm pockets, minor radiographic bone loss, moderate bleeding on probing, and no mobility. Arestin would be appropriate for this patient because he had moderate inflammation with 4-6mm pockets. - Oral Health
This patient was classified as a Heavy based on the quantity of calculus deposits present. Calculus deposits were located supragingivally throughout the dentition, with no staining. His plaque score was fair, 1.5, with generalized accumulation. Upon interview, patient stated he used to use an electric toothbrush twice daily, but has been using a manual toothbrush after his powerbrush broke, he flosses once per week, and rinses with Listerine antiseptic. - Radiographs
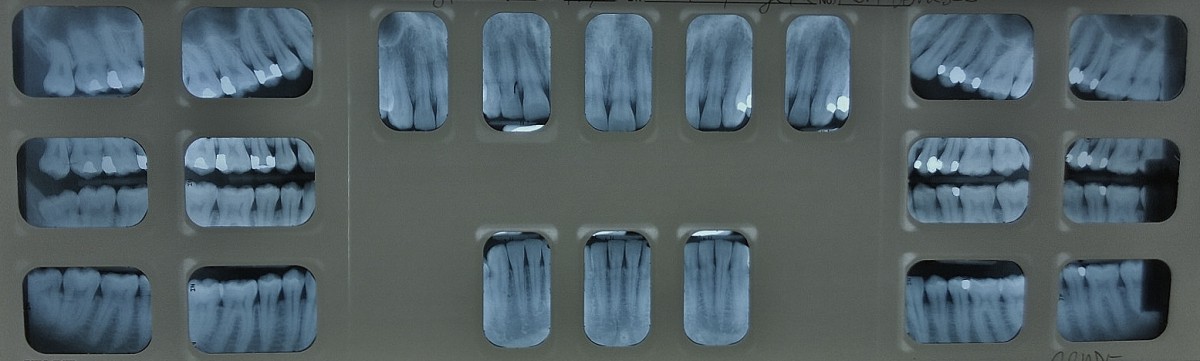
This patient required a full mouth series of radiographs which I exposed on his revisit appointment. The radiographs supported the clinical findings, and did not reveal anything additional aside from a better visual of his level of bone attachment, and rule out radiographically-visible interproximal caries.
Other Findings
This spoke no English, only Spanish, and often struggles to find the products and care he’s looking for. My Spanish is very limited so I initially tried to see if a fluent Spanish speaker would switch patients with me, but ultimately committed to the task. I printed an English to Spanish dental term book, and studied and brought them along to the appointment. I also downloaded a translator onto my phone to help fill in the blanks. Although I tried my best to ensure the patient understood what I was asking and telling him, there were inevitably some missed opportunities. These factors may affect this patient’s outcome in reaching optimal health.
TIME: This recall appointment was 10 months since his last hygiene services. This is not an appropriate amount of time for a heavy type patient. A more appropriate time interval for a chronically heavy case patient would be a 3 month recall, to keep his oral hygiene under stricter management and prevent the progression of periodontal disease.
TREATMENT MANAGEMENT: On the first visit, I gave oral hygiene instructions to the patient, and scaled his upper right and lower right quadrants. On the second (and final) visit, I exposed a full mouth series of radiographs, reviewed oral hygiene instruction and scaled his upper left and lower left quadrants, polished, flossed, and applied 2.5% NaFl foam. Upon his return home, I recommended the patient discard his toothbrush and use the one I provided to him and continue with soft-bristled brushes from thereon. I taught him the modified bass technique and stressed that he avoid lateral brushing especially on the mandibular facials, and to use a gentler amount of pressure while brushing. I also recommended he look at what electronic toothbrushes are available in England, and consider switching to an e-brush for more efficient toothbrushing. I encouraged the patient to floss daily, to brush or scrape his tongue, and to look for a fluoride-based mouthrinse to use at home instead of the Corsodyl. I made the patient aware of his carious lesions and how his frequent diet soda, and sugared tea ingestion impact the frequency and progression of those lesions, and ma sure he understood he needed to both implement a source of fluoride into his daily routine and decrease the frequency he drinks acidic and sugary beverages. The patient was given a referral, along with a copy of his xrays, for caries evaluation of #2, 11, 12, and 30.
REVISIT EVALUATION: At the patient’s revisit appointment, his plaque score decreased to a 0.3. This appointment was only 2 days after his initial appointment, but he said he had implemented the new brushing technique, and flossed since his last visit. His gingival tissue was still red, with pale margins, bulbous, and spongy with no bleeding on exploring. The patient showed interest in his state of improvement from first and second visits, and appeared motivated to continue with his learned techniques. He asked questions and was thoroughly impressed by the before and after visual of his mandibular anterior lingual surfaces in the mirror. At this appointment I exposed a full mouth series of radiographs, reviewed oral hygiene instruction, scaled his upper and lower left quadrants, polished with a fluoride prophy paste, flossed, and applied 2.5% NaFl foam


