

Case Study 1:
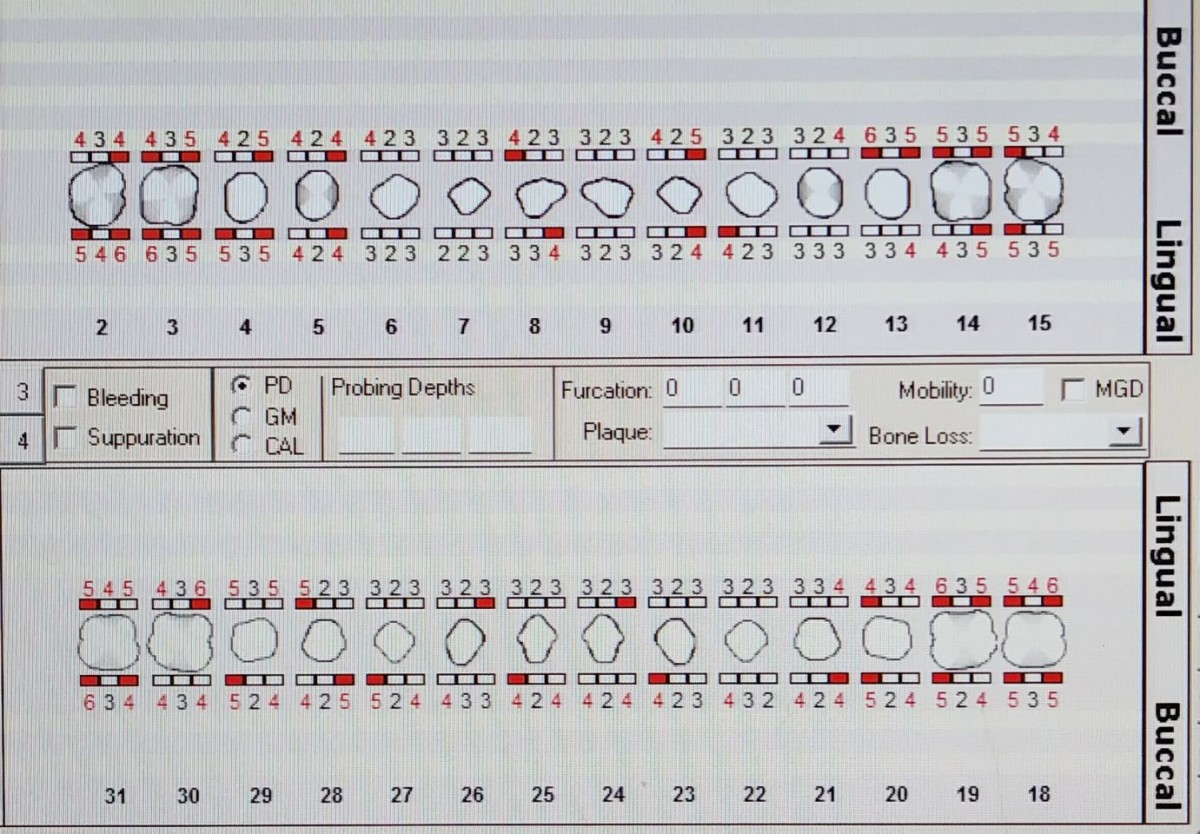
Hispanic male, 38 years of age, ASA II due to chewing tobacco use. Medium case value/Generalized Type II (2-3mm PD) and Localized Type III in posterior teeth evidence by 1-2mm recession with 5-6mm pocket depth with minimal bleeding upon exploring observed. Grade II furcation involvement #2-B, #3-B, #14-B, #15-B, revealing clinical attachment loss between 4-5mm. Red marginal gingiva with minimal inflammation on lingual surfaces of posterior teeth where the most plaque was evident. Generalized subgingival calculus on posterior teeth. Full mouth series film exposed and confirmed localized horizontal and vertical bone loss in posterior teeth about 3-4mm from the CEJ (Moderate Periodontitis).

This patient was selected for Arestin placement. Above you will find Periodontal charting pre treatment. Below you will find a detailed journal of my treatment plan which included post Arestin placement evaluation.
Case Study 2
Hispanic female, 13 years of age undergoing orthodontic treatment presented for a dental cleaning with no chief complaint. Good nutritional habits was encouraged and informed to child and caregiver. Explained moderate caries risk due to orthodontic treatment. Oral hygiene instructions were given, Charter’s tooth-brushing method and recommended purchasing an electrical toothbrush. Demonstrated how to use super floss while undergoing orthodontic treatment at least once daily followed by the use of an anticavity fluoride rinse such as ACT. After disclosing was used as a guide to demonstrate plaque and proper mechanical removal, airpolishing was used. It was determined that #18 and #31 needed sealants and it was placed using cotton roll isolation technique. After hand scaling full mouth and fine paste polish, 5 % Sodium Fluoride Varnish was applied and post instructions given.
BEFORE

2 Weeks Post Dental Cleaning

Case Study 3
Hispanic 30-year-old female, considered healthy ASA I, with a 9-month-old baby. Patient presented for a dental cleaning with chief complaint of generalized bleeding gums when brushing. She is not breast feeding and baby is only bottle feed dry formula. Last dental cleaning was 5 years ago in 2013. Generalized Type II with localized Type III perio evidenced by 6-8mm PD in posterior region with generalized red marginal and bulbous gingiva. Heavy bleeding observed while probing and exploring. Multiple amalgam restorations on molars and premolars were intact. A full mouth series was recommended and exposed, which confirmed localized bone loss on posterior teeth and inter-proximal caries #28-D. Necessary referral was given for a periodontal consultation and evaluation of #28-D. Considered a heavy case value with generalized subgingival calculus with generalized plaque observed.
Due to hormonal variations during pregnancy in conjunction with poor oral hygiene in this case caused a condition called pregnancy gingivitis. This patient was in need of oral hygiene instructions and quadrant scaling to restore her oral health. I approached this case first by informing her on her high risk for developing dental caries and educated her on baby dental health care. Emphasis was placed on informing her of the risk of vertical transmission that can harm her baby’s teeth. I recommended the use of an electrical toothbrush at least twice daily with Sensodyne toothpaste, flossing at least once a day and using Listerine Total care. During the course of 3 visits, for pain management, I administered 3% Carbocaine PSA, MSA and ASA (one carpule per visit containing 1.7ml). Ultrasonic/hand scale full mouth to completion, fine paste polish was used and 5% Sodium Fluoride Varnish was applied. Patient was given a 3 month recare date due to her heavy case value.
Before

After

Case Study 4
Pediatric 4-year-old patient was last seen by a dentist when she was 1 years old. Mother reports having a horrible experience. Child was crying and after many attempts the dental office was not successful in being able to provide care. The child was too afraid and would not open her mouth. Upon review of medical history no medical complications and patient is considered healthy. She takes speech therapy and has developed her speech enough to where she is able to communicate in small sentences. She is currently in Prekindergarten and is a shy but friendly child. Aware of the child’s past history I decided to talk to the child in the reception area before bringing her into the dental chair. After she felt comfortable enough, I walked her into the dental clinic and provided care to her cousin first while she watched. This allowed her to see what will be happening hopefully reducing her fear. The patient was able to sit in the child and open her mouth and follow easy instructions. A quick oral inspection did not reveal any suspicious caries and dentition was developing at a normal rate. I used the tell-show-do approach to provide oral hygiene instructions. Although she did not allow me to polish her teeth or neither apply Varnish, I believe that great progress was made. Hopefully, with time she will be sensitized to the dental atmosphere and will continue to make progress and allow work to be done.

Permission was granted to use photo.
Case Study 5
Hispanic, Female 19 years of age presented for a dental cleaning. Considered healthy ASA I . Generalized Type I and localized Type II perio in posterior region evidenced by 4mm PD. Generalized inter-proximal plaque and supragingival/ subgingival calculus located on the mandibular anteriors surrounding the bonded lingual retainer. She was classified as a medium case value. Oral hygiene instructions was given. Demonstrated how to properly floss underneath the bonded lingual retainer using super floss at least once a day. Also recommended brushing at least twice daily with a fluoridated toothpaste and using Listerine antiseptic twice daily.
BEFORE

AFTER

Within the intra-oral and extra-oral assessments it is essential to always be attentive to the entire oral cavity and be able to identify any abnormalities, lesions or signs of oral cancer. Here is a photograph of a benign fibroma on the maxillary frenum.

Case Study 6
Hispanic female 18 years of age, chief complaint bleeding gums while brushing, last dental cleaning three years ago. Considered healthy ASA I with no medications being taken at this time. Generalized Type I and localized Type II perio with PD 4-6 mm in posterior region mainly due to moderate inflammation, moderate bleeding observed while exploring. Bulbous gingival margins and inflamed red interdental papillae. CL II occlusion bilaterally, OJ 4mm OB 75%. Generalized plaque and subgingival calculus considered a heavy case value. Over the course of two visits quadrant scaling was performed. For pain management 1 cartridge of Oraqix (2.5% Lidocaine, 2.5% Prilocaine) per visit. My main focus was to first establish proper mechanically removal of plaque . I recommended an electrical toothbrush and demonstrated proper angulation of toothbrush head, emphasis was placed in brushing at least twice daily with a fluoridated toothpaste. I also recommended and demonstrated proper flossing technique using Reach Floss holder at least once daily followed by using Listerine Antiseptic fluoride rinse twice daily. Ultrasonic and handscaled all quadrants to completion and applied 5% Sodium Fluoride Varnish with post op instructions given. Due to severe gingivitis oral hygiene was strongly encouraged and reinforced at every visit.
Perio Charting
Patient was recommended to have a Panoramic radiograph taken to determine position and stage of development of third molars and bitewings to evaluate if intreproximal caries were evident. Radiographs revealed impacted mandibular third molars with no caries observed. Referral was given for a consultation with an oral surgeon.


Before
 AFTER
AFTER


