At first, I was skeptical towards the effectiveness of Arestin. However, this experience has completely altered my opinion. Theoretically, the use of Arestin makes sense; scaling and root planing can only do so much in deep pockets. A locally administered antibiotic is an excellent way to remove the remaining harmful microscopic bacteria, especially the red-complex bacteria. Fortunately, we were given this opportunity to experience the use of an expensive treatment aid. Initially, the patient had generalized moderate bone loss. The probing depths of the sites in which Arestin was administered ranged from 5-7mm. After allowing the antibiotic to biodegrade for four weeks, the new probing depths ranged from 3-4mm. Every site evidently improved! However, I believe it would have been easier to administer Arestin immediately after scaling was completed. If not, the gingiva would heal causing it to be firm and harder to apply Arestin. In order to create better access to the sulcus and successfully apply Arestin, I had to lavage the entire mouth to loosen the gingiva and use my instruments to flatten the tips of each cartilage. Therefore, if I were to employ Arestin in the future, I would like to do so on the day scaling was completed if radiographic evidence supports considerable bone loss. Then on the re-evaluation visit, the sites can be examined and engine polished.
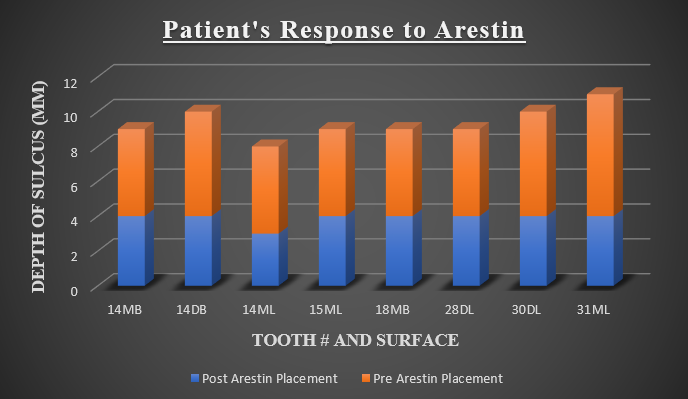
This stacked bar graph is a visualization of the patient’s response to the Arestin treatment.

