Case Study #1–HBP CASE
Initial Visit: A 31-year-old female came to our clinic for deep cleaning as recommended by her dentist. Her BP was 136/80 which corresponds to Stage 1 hypertension. Pt is also allergic to seafood and takes Zyrtec when needed. Discussed with pt about her BP and was informed that her mother also has HBP. Gave out a referral for her to consult with her physician. ASA 2 patient. The last time the patient got her x-rays, cleaning, and check-up was a month ago before she came to this clinic. Pt reports that she uses Philip’s Sonicare electric toothbrush 2x a day, uses floss every day, and uses mouth rinse occasionally.
Upon checking her EO, there was a swollen left mandibular lymph node that was discussed with the patient. From dental charting, there were some composite restorations and some suspicious decay that was also discussed and given a referral.
Localized PD of 7 was noted on the mandibular molar with a generalized PD of 5-6mm. She was classified as a Stage II, Grade B according to PD. Completed flossing technique where the patient was able to demonstrate it back, completed scaling quad 1.
Second Visit: BP was 118/97 which corresponds to Stage 2 Hypertension. Waited 20 minutes to retake BP and it was still the same. Pt informed us that she visited her physician since the last visit and was prescribed Lisinopril (10 mg 1x a day). She also got a referral to see a nephrologist because the physician was worried that there might be some problems with her kidneys. Told the patient that we need medical clearance in order to treat her. No treatment was done, pt was dismissed.
Third Visit: Pt came with clearance from her nephrologist and reported that she has been diagnosed with chronic kidney disease. She was prescribed simvastatin (5 mg 1x a day). Rechecked quad 1, and noted less inflammation and BOP. Oraquix was administered to scale quad 3+4 and pt tolerated the procedure. Recommended patient to use the proxy brush for her gums.
Fourth Visit: BP was 125/80. Pt likes the proxy brush and started to floss more as well. Revisited quad 3+4, pt had no tissue trauma, no residuals, and pt presented with less inflammation. Oraquix was used for quad 2 and completed engine polishing and fluoride.
Takeaway: This was a very eye-opening case because it reminded me again how it is crucial for us as hygienists to give referrals not only to peridontitis, or oral surgeons for the teeth but to the physicians so that we can make sure that they are healthy overall. If it hasn’t been for the referral, she might not have discovered that she has Chronic Kidney Disease.
Case Study #2- Stage IV Perio Case
A 41-year-old Asian male comes to the clinic for deep cleaning. Pt reports smoking for 10 years. No meds, no allergies reported. BP was within the normal range.

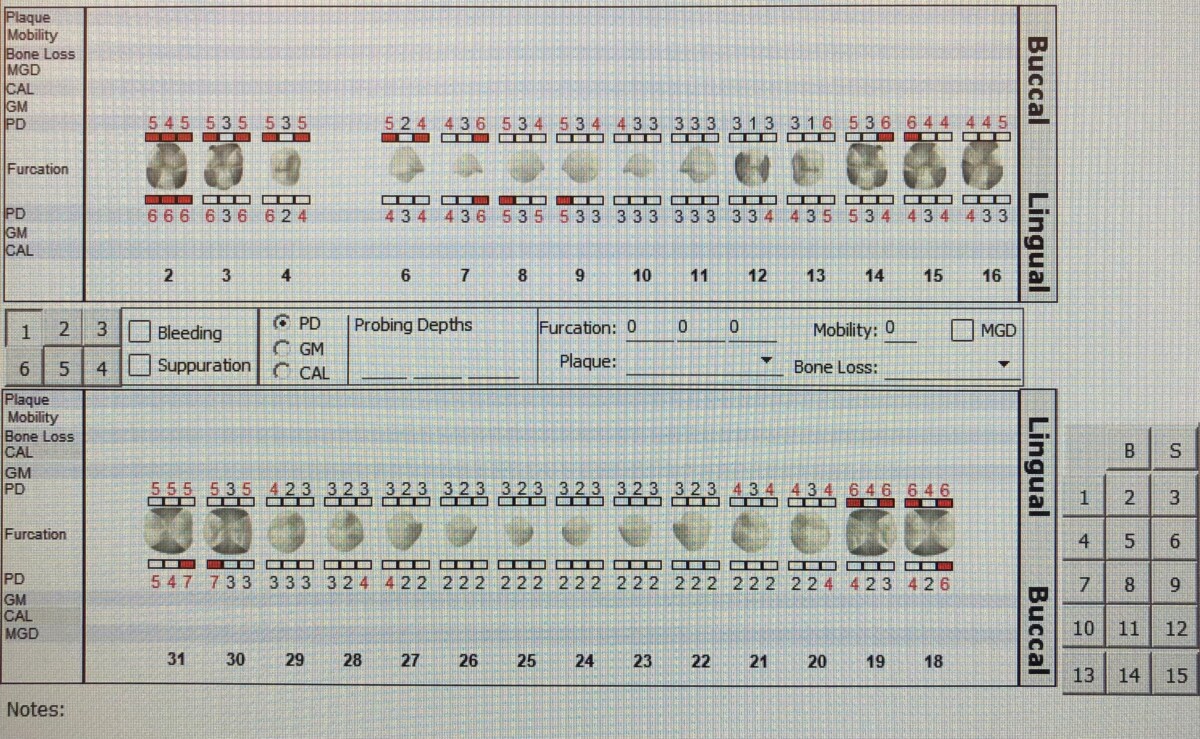
Perio chart reveals mobility on the mandibular arch, pt has generalized severe BOP. Pt has localized recession on the linguals of the mandibular anteriors. Pt has generalized PD of 5-6 mm with localized 7 mm.
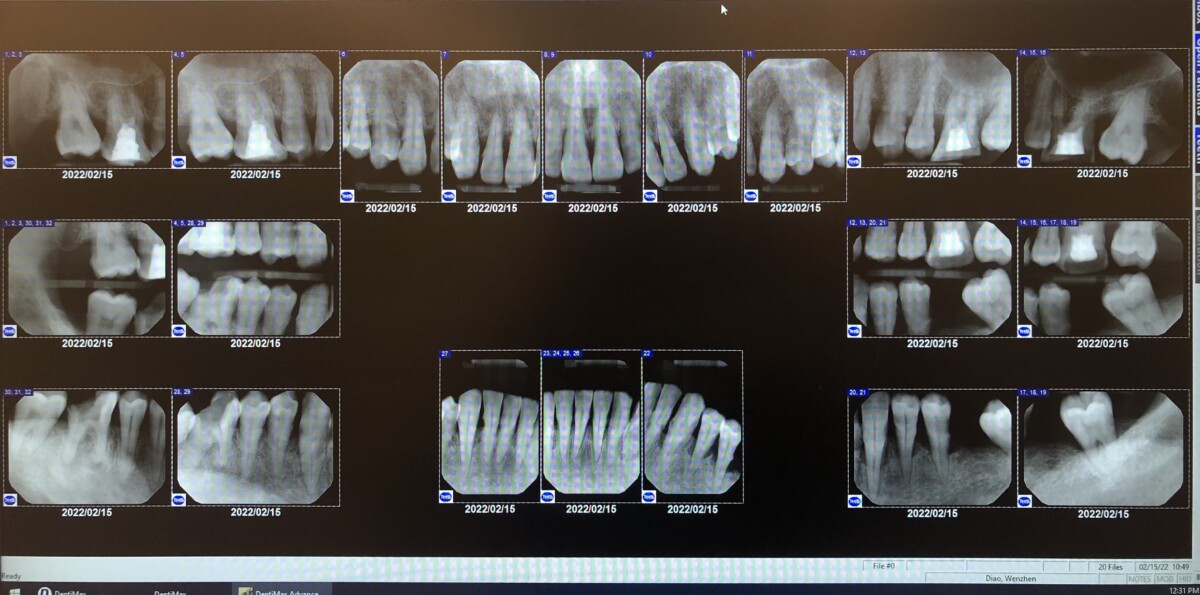
FMS reveals severe bone loss of more than 50%, especially on the lower anteriors.
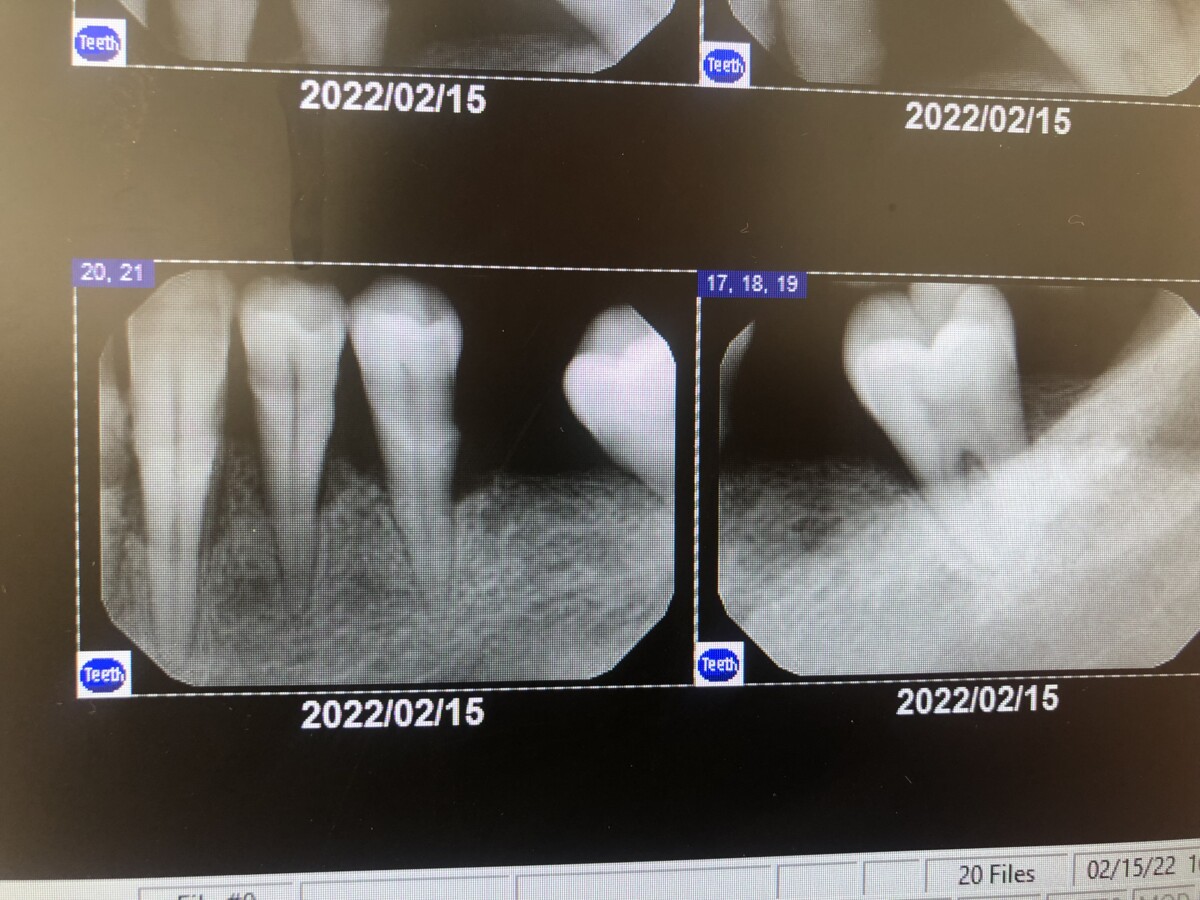
Discussed radiographic findings with the patient, gave a referral to a periodontist, and dismissed the patient.
Case Study #3-Arestin Case
A 28-year-old Asian female comes to the clinic for deep cleaning. She complains of bleeding every time she brushes with her electric toothbrush. No meds, allergies, ASA 1.

Generalized severe BOP, localized 7 mm on the maxillary anteriors, radiograph was needed to see RBL.
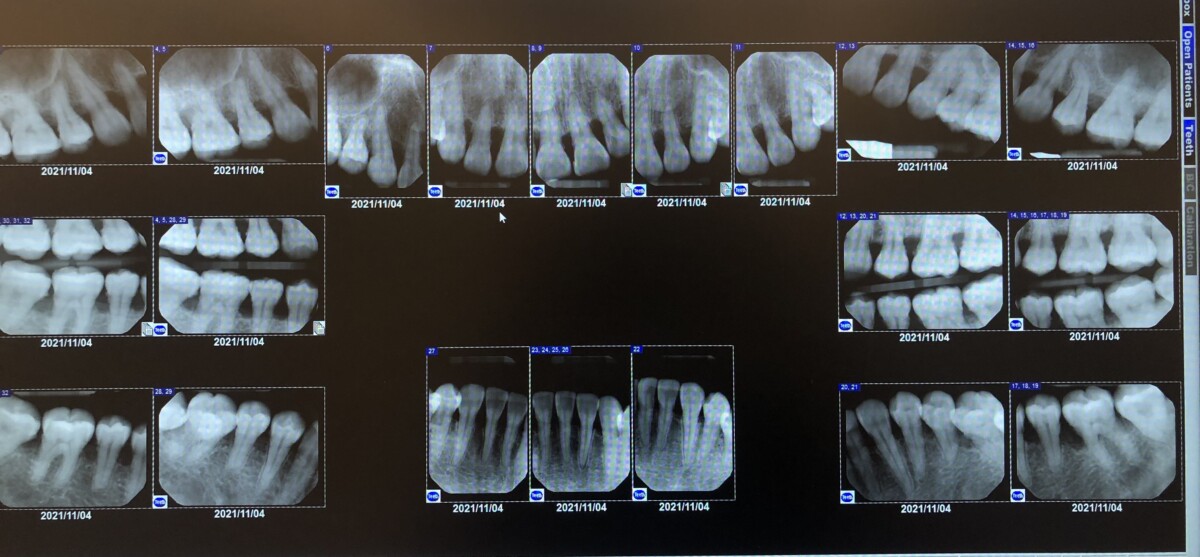
Radiograph shows generalized horizontal bone loss >33% with calculus noted as well. Discussed with patient and decided to place arestin on 4 sites.
- #3-D:6mm
- #7-M:7mm
- #8-M:6mm
- #8-D :7mm
After all the scalings were completed in all quadrants, placed arestin and did reevaluation on those 4 sites 4 weeks later. Informed pt of arestin instructions and pt was able to follow.
New PD was recorded as:
- #3-D:5mm
- #7-M:4mm
- #8-M:5mm
- #8-D :5mm

