Arestin placement
Mr. RN is a 53yo European male. He had regular visit to the dentist but never got a deep cleaning. The first visit was on June 2021, where a full medical intake and dental examination was performed. Mr. RN was a ASA 2 due to being allergic to Aspirin and Ibuprofen.
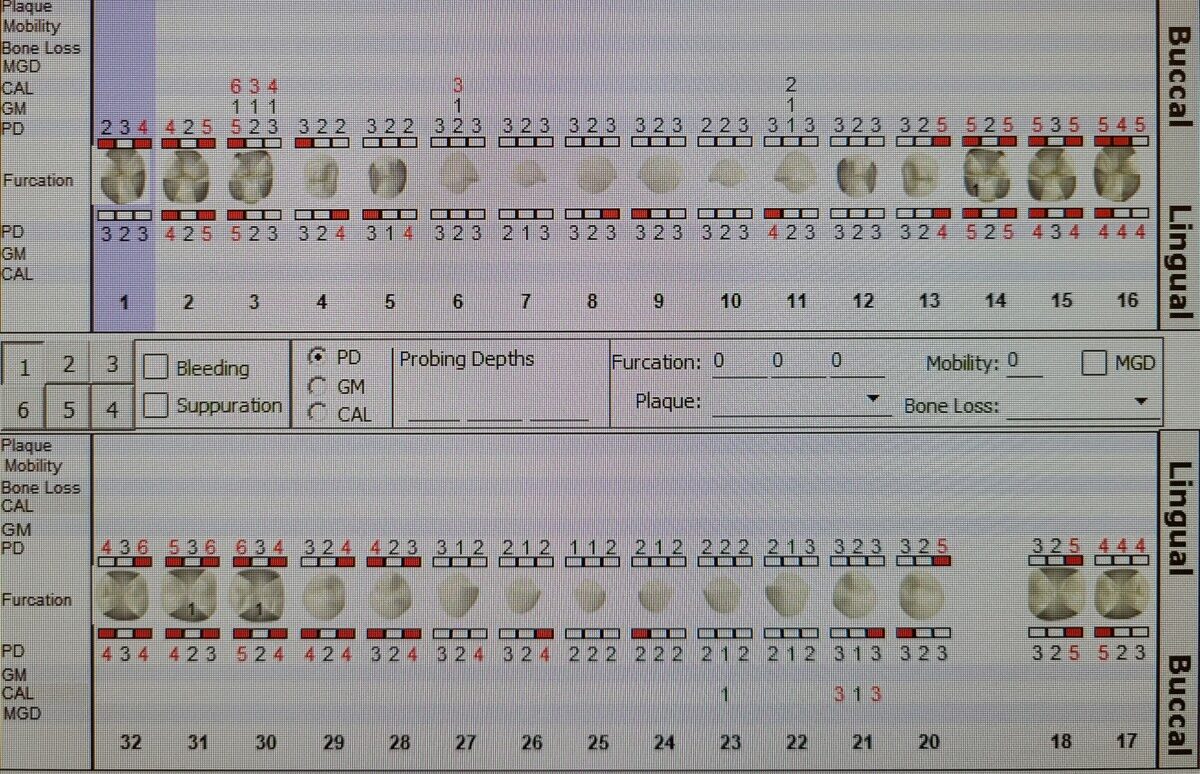
He presented generalized moderate gingival inflammation with moderate redness on mandibular anterior teeth. The papilla was bulbous, the texture shiny and moderate BOP was present mostly on posterior teeth. The periodontal chart showed PD of 1-4mm on anterior teeth and 4-6mm on posterior teeth. Teeth #2 and #15 were not probe because of patient exhibiting pain on that area. An FMS was also exposed on the visit. The radiographic and clinical findings categorized the patient as Stage II, grade B of Periodontitis. The patient showed generalized 20% horizontal bone loss. The treatment plan was a complete scaling of the mouth and a recare visit in 4 months.

The recare visit was on November 2021. Mr. RN exhibited a positive change in his gingival health, with less inflammation and marginal redness. The new periodontal exam had PD of 1-3 on anterior teeth and 4-5mm on posterior teeth with 3 pockets of 6mm on #30-D, #31-M and #32-M. After the improvement in the oral health of the patient; the instructor and I saw the use of Arestin (minocycline HCl) on the 3 pockets mentioned above, a good option for the patient. I placed the Arestin (minocycline HCl) in the pockets and gave the patient the post-op instructions.
The following recare visit was on March 2022. The patient had mild gingival inflammation on mandibular anterior teeth with localized redness on the lingual aspect. The overall PD on the updated periodontal exam indicated a an improvement. The patient had an extraction of #32 as result of sensitivity and pain. The PD of #30-D and #31-M decreased from a 6mm to 4mm.


